
Translate this page into:
Organ-preserving enucleation in a case of solid pseudopapillary neoplasm of pancreas

*Corresponding author: Arka Banerjee, Department of Pediatric Surgery, B J Wadia Hospital for Children, Mumbai, Maharashtra, India. arkabanerjee6989@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Karkera P, Banerjee A, Munghate G, Bendre P. Organ-preserving enucleation in a case of solid pseudopapillary neoplasm of pancreas. Wadia J Women Child Health 2023;2(2):86-8.
Abstract
Solid pseudopapillary neoplasm (SPN) is a rare pancreatic tumor affecting mostly females in the second or third decade of life. These tumors have a low malignant potential, and hence, surgical resection remains the main treatment. Large tumors may present with compressive symptoms such as abdominal pain or vomiting. Once resected completely, SPNs usually have an excellent long-term prognosis. We report a 16-year-old girl who presented with vomiting and abdominal pain localized to the right upper quadrant. Imaging showed an encapsulated tumor arising from the pancreatic head which prompted us to perform organ-preserving enucleation. Histopathology confirmed the tumor as an SPN.
Keywords
Solid pseudopapillary neoplasm of pancreas
Solid pseudopapillary tumor
Pancreatic tumor
Frantz tumor

INTRODUCTION
Solid-pseudopapillary neoplasm (SPN) of the pancreas was first described by pathologist Frantz in 1959.[1] It is considered a rare pathologic entity with low malignant potential, affecting mainly young females. It accounts for 0.13–2.7% of exocrine tumors of the pancreas.[2] In 1996, the World Health Organization (WHO) defined it as “solid pseudopapillary tumor” of the pancreas.[3] Before that, this tumor was known by different names such as “solid cystic tumor,” “papillary cystic tumor,” “papillary epithelial neoplasia,” “solid and papillary epithelial neoplasia,” “papillary epithelial tumor” and “Frantz’s tumor,” “solid and papillary tumor,” “solid-cystic papillary epithelial neoplasm,” and “benign or malignant papillary tumor of the pancreas.” Although they have low malignant potential, they can invade locally. However, recurrence is unusual following complete surgical resection.[2] We report a case of an 18-year-old girl who presented with abdominal pain and vomiting and was diagnosed with a pancreatic SPN which was successfully excised.
CASE REPORT
An 18-year-old girl presented with multiple episodes of non-bilious vomiting for the past 20 days. She also complained of vague, dull aching upper abdominal pain since 2 weeks. On clinical examination, there was a palpable lump in the right upper abdomen. On ultrasonography, there was a large well-defined solid cystic mass in the pancreatic head region, measuring 11 × 9.8 × 7.7 cm, with peripheral calcific foci. A contrast-enhanced computed tomography (CT) scan of the abdomen revealed a well-demarcated ovoid solid cystic lesion in the retroperitoneum, 14 × 10.5 × 14.9 cm in size, closely related to the pancreatic head. The tumor compressed the distal common bile duct with mild upstream prominence of the intrahepatic biliary radicals. A CT-guided biopsy from the mass lesion was suggestive of a solid pseudopapillary neoplasm of the pancreas. On exploration, we found a large solid, cystic neoplasm arising from the pancreatic head, adherent to the middle colic vessels in the transverse mesocolon, and the inferior mesenteric vessels [Figure 1]. The mass was enucleated in toto, carefully safeguarding all the vessels, and the mesocolic defect was closed [Figure 2]. Post-operative recovery was uneventful. The histopathological examination confirmed the presence of cells in a solid and pseudopapillary pattern which were positive for β-catenin, CD10, CD56, synaptophysin, chromogranin, and CD99. The tumor margins were clear with no extracapsular or lymphovascular spread and no involvement of surrounding lymph nodes. The patient is doing well after 2 years of follow-up.
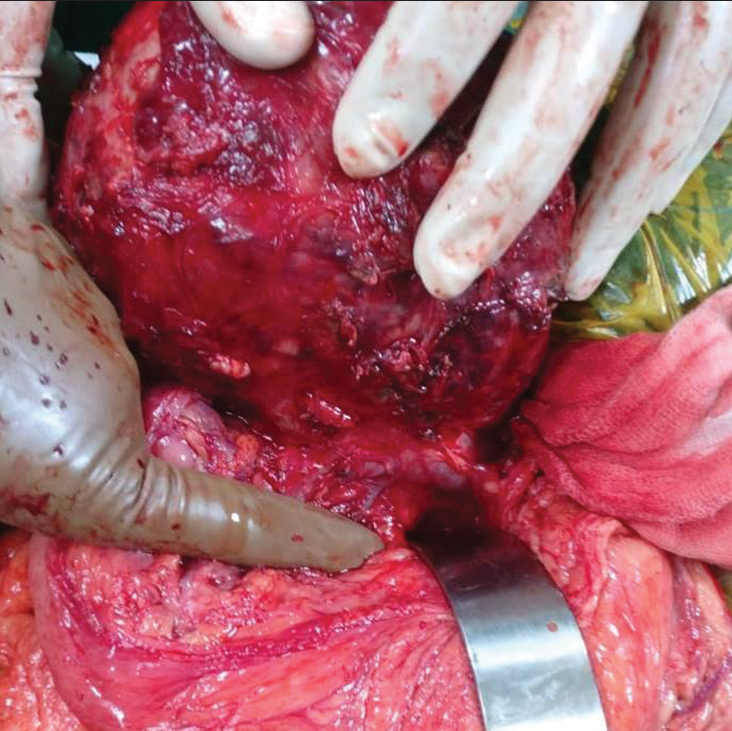
- Pancreatic mass closely adhered to middle colic and inferior mesenteric veins.
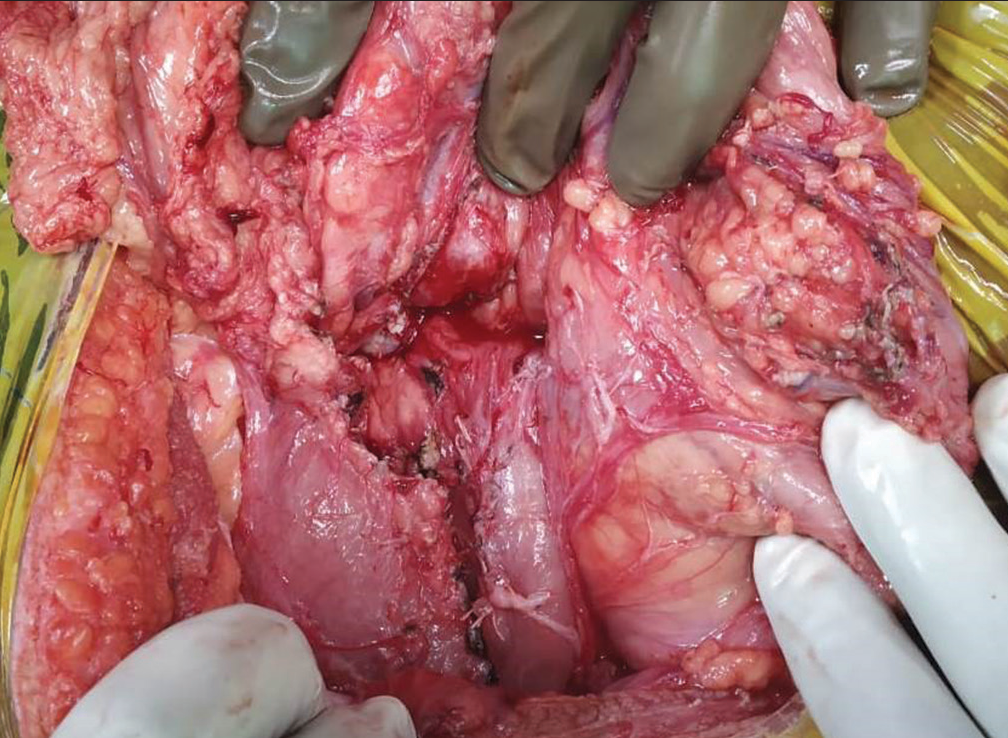
- Pancreatic bed after enucleation of the mass.
DISCUSSION
Solid-pseudopapillary neoplasm, is an epithelial tumor of pancreas with low malignant potential that predominantly occurs in young women. The usual age of presentation is the second or third decade of life with a ten-fold higher incidence in females. Around one-fourth of the cases are seen in children.[2]
The WHO classifies SPNs into two types – SPN with uncertain potential for malignancy and a solid pseudopapillary carcinoma (SPC). The criteria that distinguishes potentially malignant tumors, classified as SPC are perineural invasion, angioinvasion, deep invasion into the surrounding tissue, and distant metastases.[3,4] The origin of this tumor is unclear. Kosmahl et al. suggested it to be extra pancreatic genital ridge angle-related cell origin rather than a ductal epithelial, and neuroendocrine origin or multipotent primordial origin as thought earlier.[5]
The clinical presentation of SPNs is with non-specific symptoms such as abdominal discomfort, mild abdominal pain, or asymptomatic palpable lump or incidentally diagnosed abdominal mass on imaging. Some patients may present with obstructive symptoms such as nausea, vomiting as in our case or jaundice.[2,6] CT scan, ultrasonography, endoscopic ultrasound, and magnetic resonance imaging are the various imaging modalities used to diagnose SPN. The typical appearance on CT is that of a large encapsulated pancreatic mass with well-defined borders that contain areas of calcifications as well as intratumoral hemorrhage.[7] The most common location of SPN is the tail of the pancreas, followed by the head and the body of pancreas.[2,7] About 85% of SPNs are localized to the pancreas while around 15% have already metastasized at presentation.[7,8] Unusual presentations include multicentric tumors in the pancreas and extrapancreatic sites, such as the mesocolon, retroperitoneum, omentum, liver, and duodenum, possibly representing synchronous tumor spread. Hematological investigations and tumor markers are usually unremarkable.[9,10]
Complete surgical resection is the treatment of choice. In view of its low malignant potential, organ preserving surgery is preferable. Even though SPNs may present as large sized masses due to delayed diagnosis, tumor size is not a predictor of resectability. The various surgical options include Whipple’s pancreatoduodenectomy, distal pancreatectomy (with or without splenectomy), middle pancreatectomy, or enucleation depending on the size, location, and invasion of adjacent vessels and organs.[2,9,10] Follow-up becomes essential for early detection of any local recurrence or metastasis, that may occur in the liver, regional lymph nodes, mesentery, omentum, or peritoneum.
Patients with SPN have a good prognosis even in the setting of local recurrence and/or metastasis. The overall 5–8 year survival rate of SPN patients is up to 95%.[2,10] Positive tumor margins do not affect the final outcome of patients. Hence, enucleation, rather than radical resection, is advisable whenever feasible.[6,9,10] Although the role of chemotherapy and radiotherapy is unclear, it has been used in some cases with aggressive disease.[11,12]
CONCLUSION
SPN is a rare pancreatic neoplasm that typically affects young females with vague symptoms. Appearance on cross-sectional imaging is characteristic and a pancreas-conserving surgical approach is advisable as these patients have an excellent long-term survival, even with positive resection margins, local recurrence, and/or metastasis.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Tumors of the pancreas In: Bumberg CW, ed. Atlas of Tumor Pathology, VII, Fascicles 27 and 28. Washington: Armed Forced Institute of Pathology; 1959. p. :32-3.
- [Google Scholar]
- Solid pseudopapillary tumors of the pancreas: Review of 718 patients reported in the English literature. J Am Coll Surg. 2005;200:965-72.
- [CrossRef] [PubMed] [Google Scholar]
- World Health Organization International Histological Classification of Tumours. Vol 2. Berlin: Springer; 1996.
- [CrossRef] [Google Scholar]
- Solid-pseudopapillary tumor of pancreas In: Bosman FT, Carneiro F, Hruban RH, Theise ND, eds. World Health Organization Classification of Tumours of the Digestive System. Lyon: IARC; 2010. p. :327-30.
- [Google Scholar]
- Solid-pseudopapillary tumor of the pancreas: Its origin revisited. Virchows Arch. 2000;436:473-80.
- [CrossRef] [PubMed] [Google Scholar]
- Solid pseudopapillary tumor of the pancreas: Experience at a tertiary care centre of Northern India. Int J Surg Case Rep. 2017;39:225-30.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis and treatment of solid pseudopapillary tumor of the pancreas. Hepatobiliary Pancreat Dis Int. 2006;5:454-45.
- [Google Scholar]
- Papillary cystic and solid tumors of the pancreas: A pancreatic embryonic tumor? Studies of three cases and cumulative review of the world's literature. Surgery. 1995;118:821-8.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis and surgical treatment of solid pseudopapillary neoplasm of the pancreas: Analysis of 24 cases. Can J Surg. 2011;54:368-74.
- [CrossRef] [PubMed] [Google Scholar]
- Solid pseudopapillary tumor of the pancreas: A review of 553 cases in Chinese literature. World J Gastroenterol. 2010;16:1209-14.
- [CrossRef] [PubMed] [Google Scholar]
- Preoperative gemcitabine for unresectable, solid pseudopapillary tumour of the pancreas. Lancet Oncol. 2005;6:185-6.
- [CrossRef] [PubMed] [Google Scholar]
- A role for radiotherapy in the treatment of solid and papillary neoplasms of the pancreas. Cancer. 1985;56:2783-5.
- [CrossRef] [PubMed] [Google Scholar]




