
Translate this page into:
A rare case of lethal Raine syndrome presenting with facial dysmorphism and pyriform aperture stenosis
*Corresponding author: Dr. Suma Sundararaju, Division of Neonatology, Department of Pediatric Medicine, Bai Jerbai Wadia Hospital for Children, Mumbai, Maharashtra, India. suma.sund@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Parsodkar A, Sundararaju S, Rao S. A rare case of lethal Raine syndrome presenting with facial dysmorphism and pyriform aperture stenosis. Wadia J Women Child Health 2022;1(1):27-8.
Abstract
Raine syndrome is a very rare autosomal recessive disorder characterized by osteosclerosis, periosteal bone formation and distinct facial abnormalities that include microcephaly and low set ears osteosclerosis, cleft palate, gum hyperplasia, broad and depressed nasal bridge and proptosis. Patients affected with this syndrome have a mutation in FAM20C gene located on 7p22.3. This gene is responsible for phosphorylation of Serine residues on an enzyme casein kinase which helps in mineralisation of the bones.
Keywords
Raine syndrome
Osteosclerosis
Pyriform aperture stenosis
FAM20C

INTRODUCTION
This is a case of genetically proven Raine syndrome (RNS)[1] of lethal variety who presented with respiratory distress and dysmorphic facies.
CASE REPORT
We report a female neonate born to third degree consanguineously married couple at 37 weeks gestation and weighing 2.7 kg at birth. The mother is a 28 years old healthy female primigravida with an uneventful antenatal period. Antenatal ultrasound scan done at 34 weeks gestation was suggestive of pulmonary valve stenosis, oligohydramnios and osteogenesis imperfecta. The baby was born via caesarean section in view of non-progression of labour and had a weak cry at birth. In view of respiratory distress since birth and multiple anomalies the baby was referred to our hospital. Since admission the baby was tachypneic with suprasternal, subcostal and intercostal retractions and bilateral rales. She was initially put on non-invasive ventilation but then required invasive ventilation in view of worsening distress. Other systemic examination findings were normal. Dysmorphic features were seen in the form of a wide and bulging anterior fontanelle, narrow and prominent forehead, dolichocephaly, craniosynostosis, proptosis and hypertelorism, hypoplastic nose, low set ears, micrognathia, hypertrophic gums and short neck [Figure 1a]. Fundus examination was normal. Bronchoscopy was done which showed bilateral nasal obstruction right more than left and Type 3 laryngotracheomalacia. Infantogram of the baby showed generalised osteosclerosis [Figure 1b]. Neurosonography showed extensive periventricular echogenicity seen in frontal, parietal, temporal and occipital regions. CT scan of paranasal sinus showed hypoplastic bone of mid face, severe pyriform aperture stenosis [Figure 1c], intracranial calcifications along periventricular white matter and basal ganglia [Figure 1d]. MRI brain was also done suggesting microhemorrhages in posterior periventricular white matter. Other routine and blood investigations were within normal limits. The features of osteosclerosis, pyriform aperture stenosis, intracranial calcifications and the dysmorphism[2] raised the suspicion of RNS and whole exome sequence was sent to confirm the same. Baby was managed with intravenous antibiotics and enteral feeds. Palliative counselling was done and the prognosis of the child explained to the parents. Patient succumbed to respiratory failure on 15th day of life. On follow up the result of whole exome sequencing showed mutation in FAM20C[3] gene diagnosing RNS of lethal variety. Being autosomal recessive in nature parents have been advised genetic testing before planning the next pregnancy.
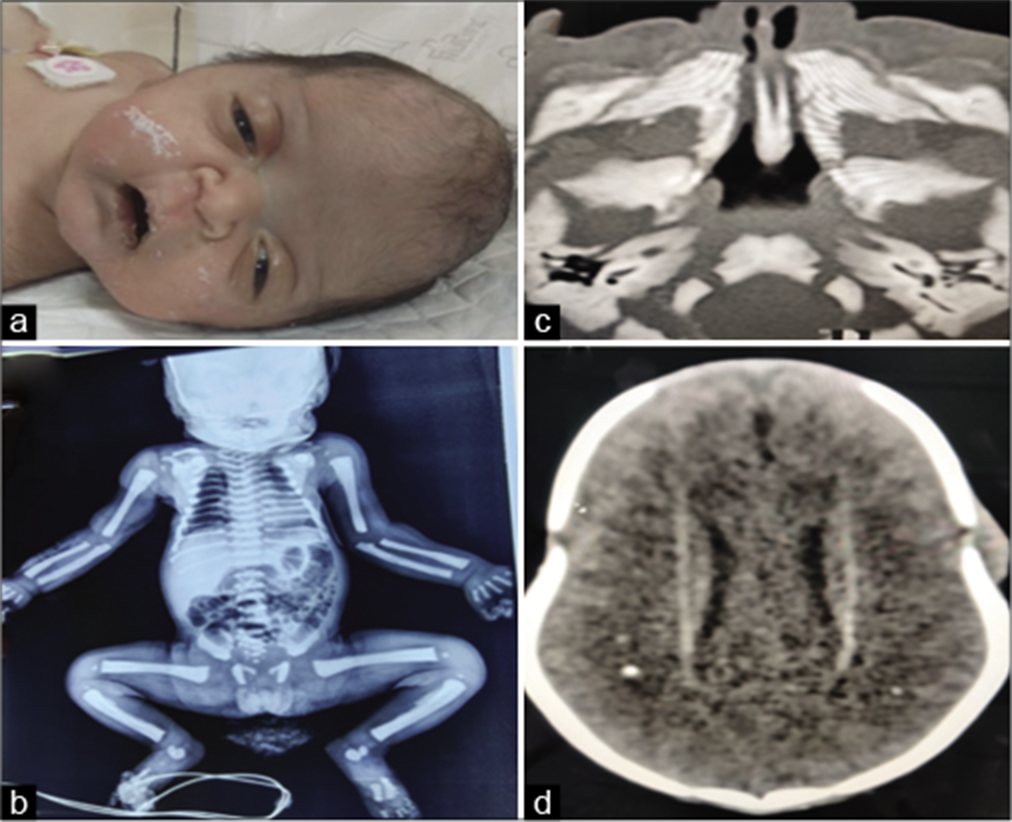
- (a) The distinct facial features of Raine syndrome. (b) Generalized osteosclerosis with periosteal bone formation. (c) Pyriform aperture stenosis on CT PNS. (d) Intracerebral calcifications on NCCT brain.
DISCUSSION
RNS (aka osteosclerotic bone dysplasia) is a rare autosomal recessive disorder with characteristic features of exophthalmos, choanal atresia/stenosis, osteosclerosis and cerebral calcifications. It is caused by biallelic loss of function mutations of FAM20C (molecule which phosphorylates caseins and proteins needed for biomineralization). Lethal and non-lethal[4] variants are known. Hypophosphatemic rickets is seen in non lethal variants due to upregulation of FGF 23. Cerebral hyper-echogenicity and distinct facies when present simultaneously on antenatal scans are highly suggestive of RNS. Management should focus on the respiratory problems, which can be fatal. Long term multidisciplinary surveillance is recommended to manage and support development, growth and to improve long term prognosis.
CONCLUSION
Our case was a lethal variety of Raine syndrome although non lethal milder phenotypes have also been reported. Facial dysmorphism and striking radiological findings should prompt towards early diagnosis of this syndrome.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Natural history of non-lethal Raine syndrome during childhood. Orphanet J Rare Dis. 2020;15:93.
- [CrossRef] [PubMed] [Google Scholar]
- A case of Raine syndrome presenting with facial dysmorphy and review of literature. BMC Med Genet. 2018;19:76.
- [CrossRef] [PubMed] [Google Scholar]
- Nonlethal raine syndrome in a newborn boy caused by a novel FAM20C variant. Mol Syndromol. 2021;12:169-73.
- [CrossRef] [PubMed] [Google Scholar]




