
Translate this page into:
Not just a hypocalcemic seizure: DiGeorge syndrome
*Corresponding author: Dr. Zainab Gilitwala, Department of Pediatrics, Bai Jerbai Wadia Hospital for Children, Mumbai, Maharashtra, India. drzainabgilitwala1912@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gilitwala Z, Joshi R. Not just a hypocalcemic seizure: DiGeorge syndrome. Wadia J Women Child Health 2022;1(1):18-20.
Abstract
DiGeorge syndrome is a spectrum of disorders characterized by the malformation of the third and fourth pharyngeal pouches. It is a hereditary disorder caused primarily by chromosome 22 microdeletions. We present a case of a 2-year-old boy who suffered from recent onset generalised seizures. The cause of the convulsions was determined to be severe hypocalcaemia. The child had dysmorphic facies, delayed language development, and an acyanotic heart disease. These observations resulted in clinical suspicion of Di George syndrome, which was confirmed using fluorescence in situ hybridisation. The clinical range of 22q11 deletion syndrome is broad, as evidenced by this patient’s results.
Keywords
Hypoparathyroidism
Rickets
DiGeorge

INTRODUCTION
In 1965, Dr. Angelo Digeorge coined the term “Di George syndrome.” The prevalence of this illness is believed to be between 1 in 3000 and 1 in 6000 people.[1] Although autosomal dominant inheritance has been recorded in 10–20% of individuals, the inheritance is frequently sporadic.[1] Microdeletions resulting in a polymorphic presentation are well known in the 22q11.2 deletion syndrome (22q11DS). Cardiac and palatal abnormalities, immunological dysregulation, hypoparathyroidism with development, and behavioural issues are the most common symptoms of this condition. However, owing to its broad clinical spectrum, 22q11 deletion identification in children without typical symptoms can be delayed. We present the case of a 2-year-old child who had seizures owing to hypocalcaemia with underlying hypoparathyroidism and was diagnosed with 22q11DS.
CASE REPORT
A firstborn 2-year-old male child born of nonconsanguineous marriage presented to our hospital with chief complaints of multiple episodes of generalized seizures with no postictal drowsiness. There was no history of fever, altered sensorium, or evidence of focal neurological deficit. His birth and antenatal history were normal and the family history was unremarkable. The child had language delay with normal hearing. At 2 years of age he could only say monosyllable words. The other development milestones were normal. He also had a history of behavioural abnormalities in the form of aggressive behaviour and poor social interaction. His birth and family history were not significant. In the past, he was admitted for an episode of pneumonia at 1 year of age.
On examination, his growth centiles of height for age and weight for age were between 3rd and 50th centile, he also had coarse facies which included hooded eyelids with upslanting palpebral fissures, with a bulbous nose and protuberant ears [Figure 1]. He had tachycardia with a normal blood pressure and no tachypnea. The child had a precordial bulge with a grade three pan systolic murmur loudest in the third left intercostal space in the parasternal area. He had mild hepatomegaly which was soft with rounded margins and smooth surface. The rest of the systemic examination was normal. On laboratory evaluation, the child had a normal hemogram with a normal absolute lymphocyte count. The biochemical profile was suggestive of hypocalcemia, low 25 (OH) Vitamin D, high phosphorous and normal alkaline phosphatase. The magnesium levels were normal [Table 1]. In view of low Vitamin D levels he received oral 2000 IU of cholecalciferol and calcium supplements at 100 mg/kg/day in three divided doses. The hypocalcemia persisted despite vitamin d and calcium supplementation. This led to further evaluation and it was found that parathyroid hormone levels were inappropriately normal for a low serum calcium. The child was diagnosed with latent hypoparathyroidism as a cause for the hypocalcaemia and started on 1,25 dihydroxy cholocalciferol (calcitriol) at 0.5 mg/day. His ophthalmologic evaluation was within normal limits. A chest X-ray showed the presence of thymus. 2 D echocardiography was suggestive of a small peri membranous ventricular septal defect (VSD) and a large patent ductus arteriosus (PDA). In view of congestive cardiac failure, diuretics were started, and was referred to cardiac surgeons for corrective cardiac surgery. The child is recovering well post repair of VSD and closure of PDA. The involvement of the parathyroid gland with cardiac anomalies with mild development delay and dysmorphic facies, there was a high suspicion of DiGeorge syndrome. Fluorescence in situ hybridisation analysis was sent which was suggestive of deletion of 22q11.2 [Figure 2]. DiGeorge syndrome is often associated with immunodeficiency hence, lymphocyte subset analysis was sent which was normal. Genetic counselling was done for the parents and prenatal diagnosis was explained for next pregnancy.
| Biochemical test | Values | Normal range |
|---|---|---|
| Hemoglobin | 10.2 g/dl | 11.5–15.5 g/dl |
| Total white blood cell count | 10,400 mm3 | 5000–13,000/mm3 |
| Absolute lymphocyte count | 3120/ul | 1000–5000/ul |
| Platelet count | 1.75 lakh/ul | 1.50–4.50 lakh/ul |
| Serum calcium | 3.6 mg/dl | 9–11 mg/dl |
| Serum phosphorous | 8.1 mg/dl | 3.5–6.6 mg/dl |
| Serum alkaline phsophatase | 389 IU/L | 123–469 U/L |
| Ionised calcium | 0.43 mmols/L | 1.15–1.33 mmols/L |
| Serum magnesium | 1.8 mg/dl | 1.7–2.3 mg/dl |
| S. 25 hydroxy cholecalciferol | 4.77 ng/dl | 30–100 ng/dl |
| S. Parathyroid hormone | 36.9 pg/ml | 15–65 pg/ml |
| Serum albumin | 4.0 g/dl | 3.8–5.4 g/dl |

- Characteristic clinical features (refer text).
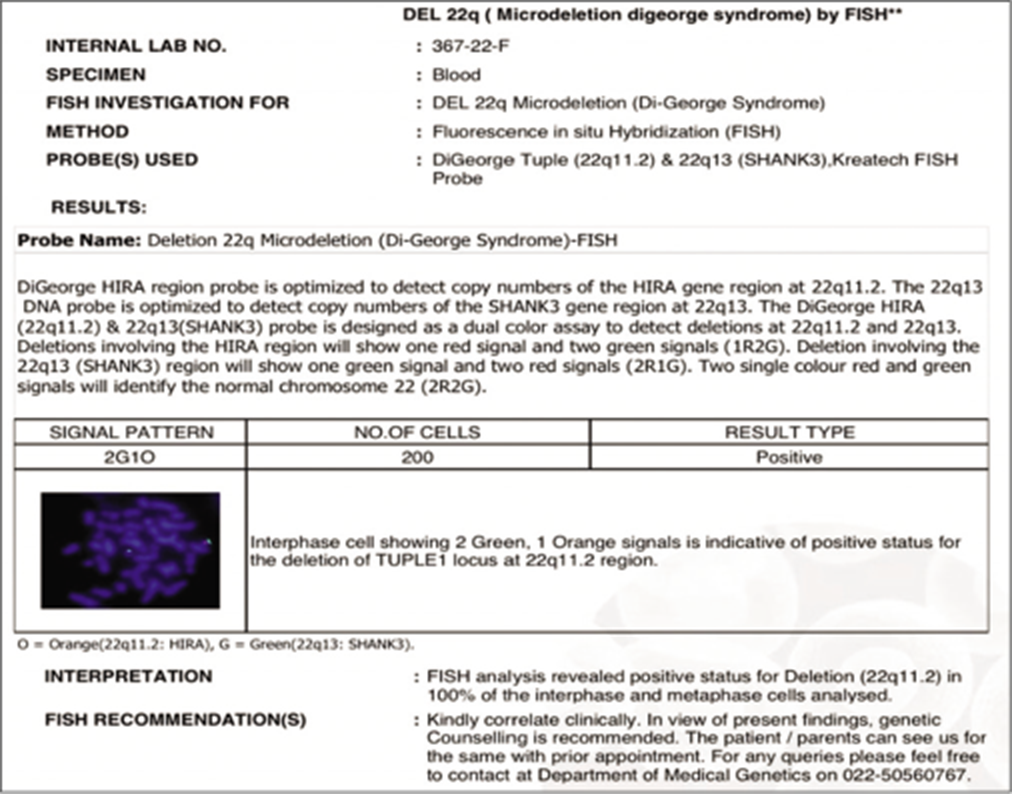
- Fluorescence in situ hybridisation analysis showing Deletion 22q 11.2.
DISCUSSION
The most frequent micro deletion syndrome is DiGeorge Syndrome, which is also the second most common cause of developmental delay and serious congenital cardiac disease.[2] It is now well established that the majority of DiGeorge syndrome patients are caused by deletions in the 22q11 chromosomal band. The area of chromosome 22q11 is extremely unstable, and misalignment of chromosome specific low copy numbers is common.[2]
The loss of the 22q.11.2 region can be caused by repeats during non allelic homologous recombination. Early morphogenesis of several organs, including the parathyroid gland, thymus, and facial tissues, can be affected by haploinsufficiency of genes located at 22q.11.2, particularly TBX1.[2,3]
Congenital cardiac disease (75%), palatal abnormalities (69%), and minor learning impairments (62%) are all part of the DiGeorge Syndrome spectrum and hypocalcaemia (60%) and immune insufficiency (70%) are due to hypoplasia of the parathyroid and thymus glands,[4,5] respectively with a wide range of severity and expression in individuals.
Hypocalcaemia was found in 60% of patients in a recent study, and it was linked to symptomatic hypocalcaemia in the neonatal era.[5] However, many patients also presented with hypocalcaemia when they were children. This suggests that hidden hypoparathyroidism is more common than persistent hypocalcaemia with symptoms.[5] In latent hypoparathyroidism, sufficient quantities of parathyroid hormone are released in basal states, and serum calcium and phosphorus levels are normal. PTH secretion becomes insufficient and hypocalcaemia develops when calcium intake is reduced, especially during periods of increasing demand such as infancy and adolescence.[6] At the onset of hypocalcaemia, our patient had poor calcium intake in diet and was also suffering from Vitamin D inadequacy. In the patient with latent hypoparathyroidism, Vitamin D insufficiency may have led to the development of hypocalcaemia. In our case, however, hypocalcemia persisted despite Vitamin D replenishment, indicating that Vitamin D deficiency was not the primary cause of hypocalcaemia.
Although patients with this disease frequently have unrecognised abnormalities, associated palatial abnormalities may not be a presenting symptom. Speech delay is frequently caused by velopharyngeal incompetence. Mild development delay was detected in 62% of cases, whereas severe learning handicap was found in 18% of cases, according to a recent study.[5]
The most common cardiac abnormalities associated with DiGeorge syndrome were conotruncal and aortic arch defects.[5,7] Tetralogy of Fallot, VSD, ASD, double outlet right ventricle, and PDA are some of the other abnormalities.[5]
The immune system is involved as a result of faulty thymus formation, which leads to improper T cell development. The majority of individuals have a modest T cell immunodeficiency.
The most prevalent renal defects in people with 22q11DS are absent, dysplastic, or multicystic kidneys. Obstructive anomalies and vesicouretetric reflux have also been discovered.
DiGeorge syndrome is frequently associated with structural brain abnormalities such as cerebral atrophy, cerebellar hypoplasia, and hypoplastic corpus callosum.
CONCLUSION
Because of its diverse presentation, DiGeorge syndrome is frequently misdiagnosed because patients appear with atypical symptoms, such as hypocalcemic seizures, as in our case. As a result, hypocalcemia due to latent hypoparathyroidism with heart defect in a dysmorphic child should elicit additional 22q11DS testing. An early recognition can aid in the improved management and monitoring of these individuals, as well as provide prenatal diagnosis for the subsequent pregnancy.
Acknowledgments
Dr. Sudha Rao Head of Department of Pediatrics, Dr. Alpana Ohri Head of Pediatric Nephrology.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A patient with 22q11.2 deletion syndrome: case report. J Clin Res Pediatr Endocrinol. 2009;1:151-4.
- [CrossRef] [PubMed] [Google Scholar]
- A Practical guidelines for managing patients with 22q11 2 deletion syndrome. J Pediatr. 2011;159:332-9.
- [CrossRef] [PubMed] [Google Scholar]
- Delayed diagnosis of 22q11 deletion syndrome due to late onset hypocalcemia in a 11-year-old girl with imperforated anus. Ann Pediatr Endocrinol Metab. 2017;22:133.
- [CrossRef] [PubMed] [Google Scholar]
- Characterstic cognitive profile in patients with a 22Q11.2 deletion-verbal IQ exceeds nonverbal IQ. Am J Hum Genet. 1995;57:42.
- [Google Scholar]
- Spectrum of clinical features associated with interstitial chromosome 22q11 deletions: A European collaborative study. J Med Genet. 1997;34:798-804.
- [CrossRef] [PubMed] [Google Scholar]
- Hypoparathyroidism as the major manifestation in two patients with 22q11 deletions. Am J Med Genet. 1994;52:478-82.
- [CrossRef] [PubMed] [Google Scholar]
- DiGeorge syndrome presenting as hypocalcaemia-induced seizures in adulthood. Case Rep Med. 2013;2013:923129.
- [CrossRef] [PubMed] [Google Scholar]




