
Translate this page into:
Bilateral complex microphthalmia with unilateral coloboma in a preterm neonate

*Corresponding author: Sruthi Nair, Department of Neonatology, Seth GS Medical College and King Edward Memorial (KEM) Hospital, Mumbai, Maharashtra, India. sruthis.doc@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bhadane A, Prashanth RR, Nair S, Haribalakrishna A. Bilateral complex microphthalmia with unilateral coloboma in a preterm neonate. Wadia J Women Child Health. 2023;2(3):148-9. doi: 10.25259/WJWCH_2_2024
A female neonate weighing 1300 g, born at 35 weeks of gestation with asymmetric intrauterine growth restriction had bilateral microphthalmia and microcornea [Figure 1] with no corneal haziness or cataracts. Fundus examination showed bilateral dysplastic retina. There were no other stigmata of intrauterine infection or any dysmorphism with normal systemic examination. B scan of the eyes showed an axial length of 14 mm in both eyes with iris coloboma in the right eye, confirming bilateral complex microphthalmia with unilateral coloboma [Figure 2]. TORCH titers, echocardiography, cranial ultrasound, skeletal survey, and automated auditory brainstem response (AABR) were normal. Parents denied genetic testing.

- Bilateral microphthalmia and microcornea.
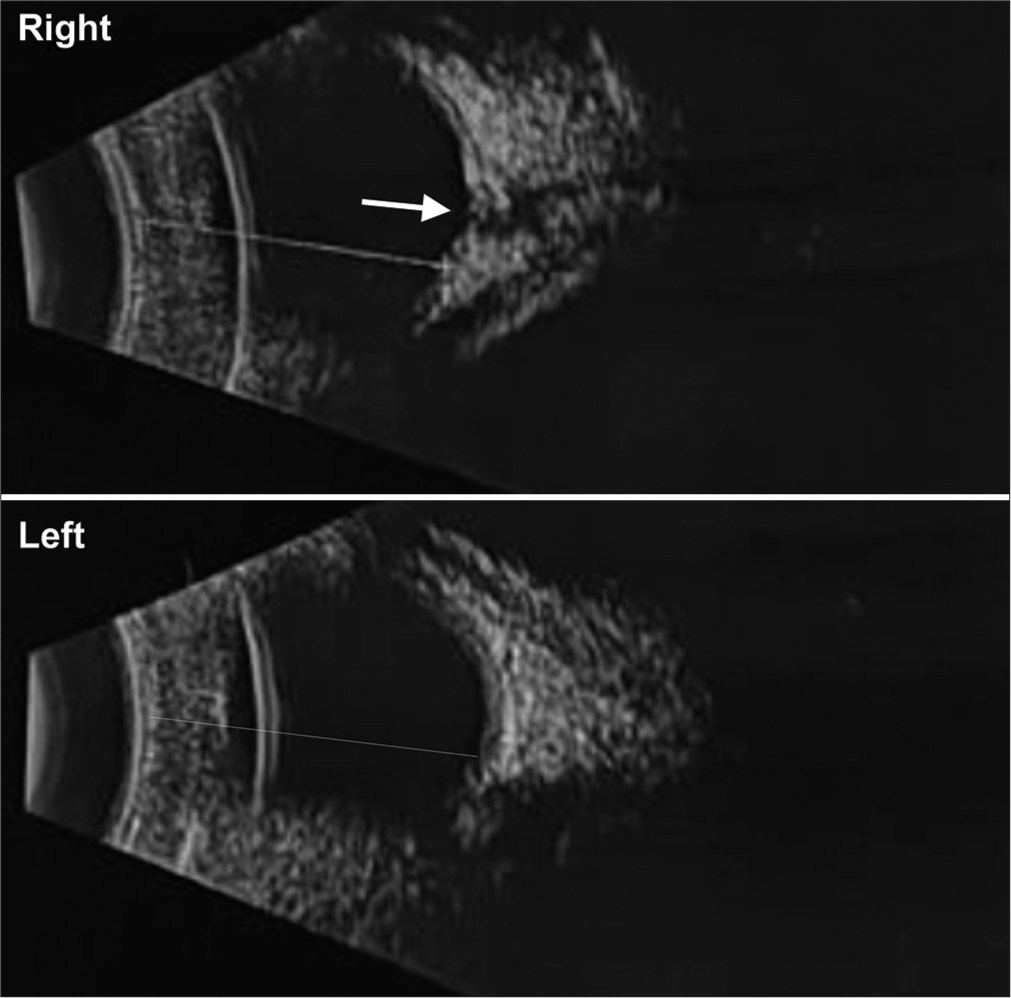
- B scan of the eyes showed a right eye axial length measuring 14 mm with iris coloboma (white arrow) and a left eye axial length of 14 mm.
Microphthalmia and coloboma arise due to defects in the optic fissure closure and are diagnosed when the anteroposterior diameter of the globe is <20 mm.[1] Rehabilitation in these complex microphthalmia (when associated with retinal dysplasia) is for cosmetic purposes and includes endo-orbital volume replacement with expandable implants or orbital osteotomies.[2]
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Anophthalmia and microphthalmia. Orphanet J Rare Dis. 2007;2:47.
- [CrossRef] [PubMed] [Google Scholar]
- Integrated reconstructive strategies for treating the anophthalmic orbit. J Craniomaxillofac Surg. 2004;32:279-90.
- [CrossRef] [PubMed] [Google Scholar]




