
Translate this page into:
Study of knowledge, attitude, and practices of child care physicians toward nutritional vitamin D deficiency in pediatric population

*Corresponding author: Ashrusha Ashok Meshram, Department of Pediatric Medicine, Bai Jerbai Wadia Children Hospital, Mumbai, Maharashtra, India. ashru.meshram16@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Meshram AA, Keshwani R, Shah D, Rao S. Study of knowledge, attitude, and practices of child care physicians toward nutritional vitamin D deficiency in pediatric population. Wadia J Women Child Health 2023;2(1):3-9.
Abstract
Objectives:
Nutritional Vitamin D deficiency (NVDD), commonly seen in infancy and childhood, is a nutritional epidemic. Practicing child care physicians have different approaches to the diagnosis and treatment of nutritional Vitamin D deficiency in children. This study aims to assess the knowledge, attitude, and practice of clinical diagnosis, investigations, and treatment of NVDD in infants and children among child care physicians from a teaching institute.
Material and Methods:
A cross-sectional study was conducted to assess knowledge, attitude, and practice of NVDD among resident doctors, consultants and faculty members working in a teaching hospital by convenience sampling method. The study was based on a pretested questionnaire which was administered by a single investigator on all the study participants. Twelve questions formulated to assess the knowledge, was scored as 0 (0%) to 14(100%) and ten questions regarding attitude and practices with possible responses as agree, disagree, or neutral was scored as 0 (0%) to 20 (100%). Data were analysed with statistical software, STATA, version 10.1,2011. Descriptive statistics included summary measures such as frequency and percentages to summarize qualitative variables and categorical responses. Inferential statistics included P-values generated from hypothesis testing procedures.
Results:
There were 96 participants including 46 residents. Forty-seven (49%) of them scored more than 11 out of 14 while 49 (51%) participants scored between 7 to 10 out of 14 on the knowledge part of the questionnaire. Interestingly nobody scored less than 7 out of 14. Sixty (62%) participants scored more than 15 out of 20 and nearly 19 (2%) physicians scored less than 10 out of 20 in the attitude and practice part of the questionnaire. On intergroup comparison between consultant pediatricians and residents on knowledge regarding NVDD showed no significant difference except for knowledge regarding cumulative therapeutic dose of cholecalciferol (p value 0.025). There were more attitude and practice gaps in this group of respondents although it was not statistically significant.
Conclusion:
This study identifies gaps in the knowledge, attitude and practice of child care physicians about NVDD in infants and children. Knowledge gaps regarding definition and change in treatment protocol of NVDD and inconsistency in clinical identification, diagnosis, treatment, and prevention protocols across all groups of physicians.
Keywords
Attitude
Children
Infants
Knowledge
Practice
Nutritional Vitamin D deficiency

INTRODUCTION
Vitamin D deficiency has been recognized as a worldwide epidemic and yet is an under-diagnosed and under-treated nutritional deficiency.[1] Nutritional Vitamin D deficiency (NVDD) is commonly seen in infancy, early childhood, and puberty which are periods of rapid linear growth. About 43.2% of infants aged 2–24 weeks suffer from Vitamin D deficiency.[2] Ekbote et al. studying Vitamin D deficiency in toddlers from Pune city found that 83% of children of study group with a mean age of 2.6 year were affected.[3]
Vitamin D, also called the sunshine vitamin, has multiple physiological roles, both skeletal and extra-skeletal. The skeletal roles are aimed at maintaining the calcium and phosphorous balance which in turn facilitates bone mineral homeostasis, musculoskeletal strength, and linear growth. The extra skeletal functions are related to its immune enhancing functions and anti-bacterial properties,[4] besides also having putative anti-proliferative and anti-tumorigenic activities in the cancer cells of the breast, colon, skin, stomach, and prostate.[5] Low levels of Vitamin D have been associated with conditions such as inflammatory bowel disease and autoimmune disorders including multiple sclerosis, inflammation,[6] chronic kidney disease,[7] various types of cancer,[5] cardiovascular disease,[8] obesity,[9] mortality,[10] Type 1 diabetes mellitus,[11] and hypertension[12] in various epidemiologic studies.
Indian socioreligious and cultural practices affect adequate sun exposure, thereby negating potential benefits of sunshine, the richest source of Vitamin D. Besides inadequate sunlight exposure, sun avoiding behavior, poor dietary source of cholecalciferol and calcium, poor maternal Vitamin D stores in an exclusively breast fed baby, and increased demands in lieu of rapid growth are some of the other confounding factors involved.
Although the incidence of NVDD is reported high in various Indian studies, the consensus on diagnosis, treatment, and follow-up care remains ever changing and often nonconfirmative. Many practicing child care physicians, especially pediatricians have different approaches to the diagnosis and treatment of NVDD in children. As there is wide variation in the diagnosis, investigation, and treatment practices, we proposed to study the varied approach to diagnosis, investigation, and management of children with NVDD by pediatricians.
The present study is undertaken to assess the KNOWLEDGE, ATTITUDE, AND PRACTICE of NVDD in children among child care physicians practicing at a teaching institute.
MATERIAL AND METHODS
Approval of the protocol and informed consent document was sought from the Institutional Ethics Committee before commencement of study.
Data were collected after informed consent, through a structured and validated questionnaire from 96 pediatricians with a minimum of 1 year working experience in the pediatric department which included faculty and residents (2nd year, 3rd year postgraduate students, and senior residents). The questionnaire was framed by the principal investigator of this study also an endocrinology expert. A pilot study was conducted in the study setting on a test sample of 10 residents and faculty as a preliminary exercise. Cronbach’s alpha was used to validate the questionnaire. The value of coefficient alpha was 0.75 from the data obtained from the pilot study which indicates good internal consistency.
The questionnaire included qualitative data consisting of 12 questions of knowledge about Vitamin D and 13 questions concerning attitude and practices. Mode of data collection was done by paper/digital questionnaire with both open-ended and closed question format. This data were evaluated by coinvestigator of the study.
Participants’ knowledge of Vitamin D was scored as 0–14 for the set of 12 question with correct answers scored as 1 and incorrect answer marked 0, except the question regarding clinical manifestations of Vitamin D deficiency for which each option was given 1 score with a maximum possible score of 3.
For attitude and practices the scoring was based on 10 questions. Answers were categorized as Agree (Score = 2), Neutral response (Score = 1), and Disagree (Score = 0). The total score range was thus 0–20.
Inferential statistics included P-values generated from hypothesis testing procedures. Overall responses were compared by qualification of the respondents in two groups, that is, Consultant Pediatricians (n = 50) versus Residents (n = 46). Then, an intragroup analysis was also performed to compare responses across three categories in the Consultant group (i.e. Fellows [n = 25], Super-specialists [n = 9] and General pediatricians [n = 16]).
Chi-square test was performed for testing difference in proportions for question-wise responses in the above independent groups.
RESULTS
Out of 96 total participants, 46 doctors are currently undergoing training as junior (2nd and 3rd year) and senior residents comprising 48% of study population. The remaining 50 (52%) respondents were consultant pediatricians who were, further categorized as fellows undergoing specialty training (26%), general pediatrician consultants/faculty members (16.6 %), and pediatric super specialists (9.4%).
Knowledge of Vitamin D
The study included 12 questions on knowledge regarding Vitamin D. About 75% (n = 72/96) of physicians were positive regarding epidemic nature of NVDD. Among the study population, 50% (n = 48/96) recognized sunlight as richest source of Vitamin D, while 49% opined it to be fish liver oil. The recommended dietary allowance (RDA) of 600 IU/day Vitamin D3 in children aged 1–18 years was known to 62.5% (n = 60/96) study population.
Majority (93.8%) of study participants agreed that breast milk is a poor source of Vitamin D. The definition of Vitamin D deficiency is based on serum 25 (OH) Vitamin D was correctly answered by 97.83% (n = 92/94) of physicians.
According to global consensus recommendations on prevention and management of nutritional rickets (2016), serum 25 (OH) Vitamin D concentration <12 ng/mL is considered deficient.[13] About 36.4% (n = 34/93) of physicians in the study opined a value <12 ng/mL to be deficient.
NVDD can be asymptomatic in many children, not always manifesting with features of rickets. About 92.71% (n = 89/96) of physician responded the same, while 7.29% opined that all children manifest with clinical features of rickets.
In our study, 39 out of 92 responders (42%) felt that treatment of NVDD was with 3.6 lac units of cholecalciferol and should be given in divided dosage as 60,000 IU weekly, while 53 of the 92 responders (57%) felt that 6 lac units should be given. About 94.75% (n = 90/95) of physicians agreed with the importance of calcium supplementation during treatment phase of NVDD.
About 46.88% (n = 45/96) of physicians have observed that bony deformities improve around 6 months after starting treatment, while 24% say that 1 year is at least required, 20% gave opinion of requiring many years for bony deformity to improve, and 9.4% physicians observed improvement in bony deformities within a month. The majority of physicians (98%) pointed out that tiredness, irritability, muscle weakness can all be manifestations of Vitamin D deficiency.
Vitamin D knowledge score distribution [Figure 1] revealed that 51% of all physicians had a score between 7 to 10 while 49% had a score above 11, with mean and median value of 10 (71.42%) out of 14.
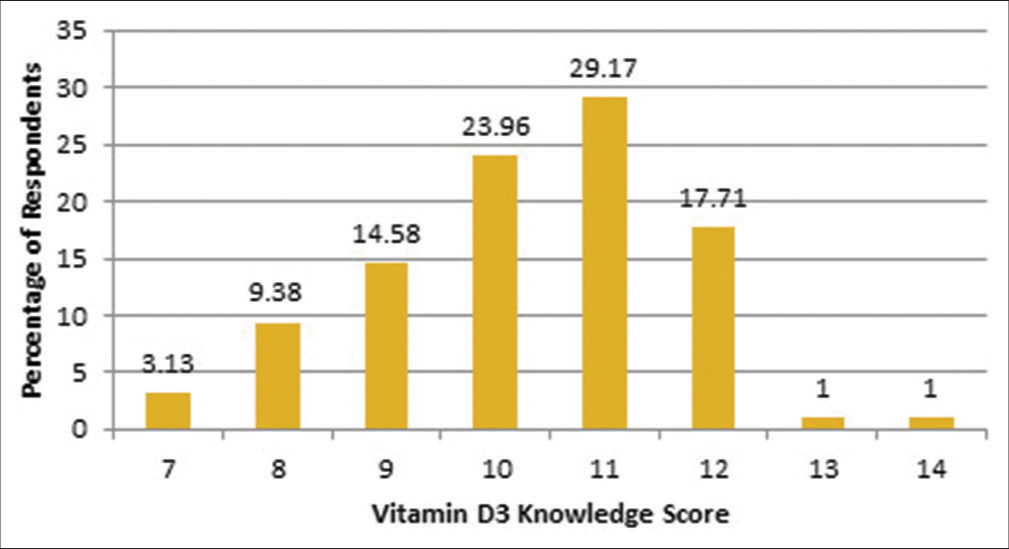
- Score of knowledge of physicians regarding nutritional vitamin D deficiency.
Intergroup comparison between consultant pediatricians and residents [Table 1] on knowledge regarding NVDD showed no significant difference except for the knowledge of cumulative therapeutic dose of cholecalciferol (P = 0.025). Intragroup comparison between fellow, general pediatricians, and pediatric superspecialists showed no significant difference [Table 2].
| S. N. | Knowledge | Resident n (%) |
Consultant Pediatrician n (%) | Total no of respondents out of 96 | P value |
|---|---|---|---|---|---|
| 1. | Nutritional Vitamin D is an epidemic | 31 (67.39%) | 41 (82%) | 96 | 0.099 |
| 2. | Richest source of vitamin D is sunlight | 20 (43.48%) | 28 (56%) | 96 | 0.307 |
| 3. | RDA of vitamin D for 1 to 18 years age 600 u/day | 33 (71.74%) | 27 (54%) | 96 | 0.168 |
| 4. | Breast milk is inadequate as source of vitamin D | 45 (97.83%) | 45 (90%) | 95 | 0.267 |
| 5. | 25(OH) vitamin D is useful in defining vitamin D deficiency | 44 (95.65%) | 48 (96%) | 94 | 0.996 |
| 6. | Vitamin D deficiency is <12 ng/mL | 17 (36.96%) | 17 (34%) | 93 | 0.804 |
| 7. | Diagnosis of rickets is made by X-ray | 24 (52.17%) | 18 (36%) | 95 | 0.405 |
| 8. | All children with NVDD do not present clinically as rickets | 43 (93.48%) | 46 (92%) | 96 | 0.781 |
| 9. | Cumulative therapeutic dose of cholecalciferol 3.6 lac IU over 6 weeks | 25 (54%) | 14 (28%) | 92 | 0.025 |
| 10. | Definite role of calcium in NVDD treatment | 44 (95.65%) | 46 (92%) | 95 | 0.583 |
| 11. | Time required for improvement in bony deformities in nutritional rickets | 22 (47.83%) | 23 (46%) | 96 | 0.922 |
| 12. | Non calcemic manifestations of NVDD | 46 (100%) | 48 (96%) | 96 | 0.17 |
| S. N. | Knowledge | Fellow n (%) | General pediatrician n (%) | Pediatric superspecialist n (%) | Total no of respondents out of 50 | P value |
|---|---|---|---|---|---|---|
| 1. | Nutritional Vitamin D is an epidemic | 21 (84%) | 15 (93.75%) | 5 (55.56%) | 50 | 0.054 |
| 2. | Richest source of vitamin D is sunlight | 10 (40%) | 12 (75%) | 6 (66.67%) | 50 | 0.069 |
| 3. | RDA of vitamin D for 1 to 18 years age is 600 IU/day | 14 (56%) | 10 (62.5%) | 3 (33.33%) | 50 | 0.683 |
| 4. | Breast milk is inadequate as source of vitamin D | 25 (100%) | 14 (87.5%) | 6 (66.67%) | 49 | 0.069 |
| 5. | 25(OH) vitamin D is useful in defining vitamin D deficiency | 24 (96%) | 15 (93.75%) | 9 (100%) | 49 | 0.533 |
| 6. | Vitamin D deficiency is < 12 ng/mL | 7 (44%) | 8 (50%) | 4 (44.44%) | 48 | 0.503 |
| 7. | Diagnosis of rickets is made by X-ray | 12 (48%) | 6 (37.5%) | 4 (44.44%) | 50 | 0.169 |
| 8. | All children with NVDD do not present clinically as rickets | 23 (92%) | 14 (87.25%) | 9 (100%) | 50 | 0.543 |
| 9. | Cumulative therapeutic dose of cholecalciferol 3.6 lac IU over 3 weeks | 9 (36%) | 3 (18.75%) | 2 (22.22%) | 49 | 0.673 |
| 10. | Definite role of calcium in NVDD treatment | 23 (92%) | 15 (93.75%) | 8 (88.89%) | 49 | 0.813 |
| 11. | Time required for improvement in bony deformities in nutritional rickets | 13 (52%) | 6 (37.5%) | 4 (44.44%) | 50 | 0.858 |
| 12. | Non calcemic manifestations of NVDD | 25 (100%) | 15 (94%) | 8 (89%) | 50 | 0.296 |
Attitude and practices regarding Vitamin D deficiency
Ten questions regarding attitude and practices with possible responses as Agree, Disagree, or Neutral were compiled to obtain a score with a range of 0–20. The response recorded is presented graphically [Figure 2].
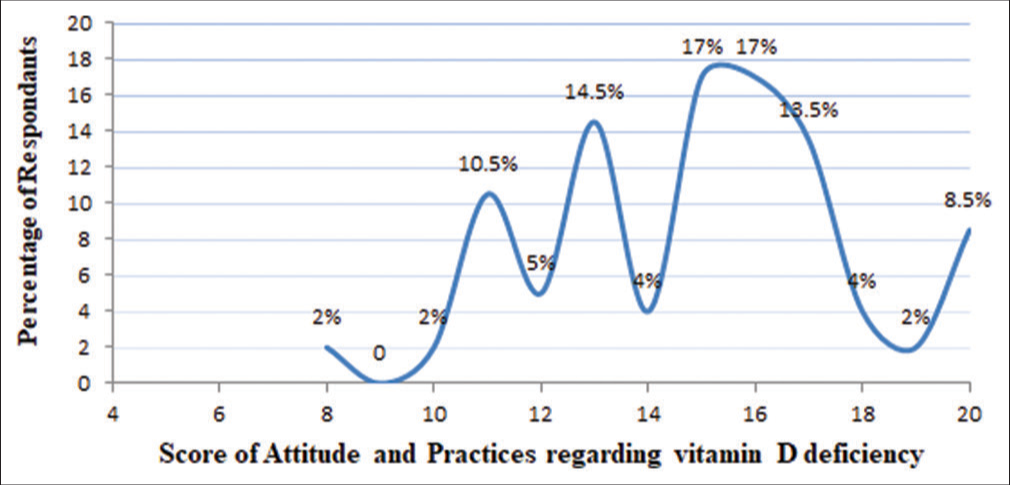
- Score of attitude and practices of physicians regarding nutritional vitamin D deficiency.
With a mean and median both of 15, 2% of physicians scored <10, 36% of physicians had a score between 10 to 15 while 62% had a score of positive attitude of >15.
About 93.4% (n = 90/95) of physicians practice to supplement RDA of Vitamin D to full term breast fed infants. About 84% (n = 77/91) of physicians do evaluate the mother and treat her, while 1% do not evaluate but treat, and 14% of physicians neither evaluate nor treat mother of child who is found to be Vitamin D deficient and is exclusively breast fed. Out of 84% of physicians who treat mother, 62.5% prescribe cholecalciferol 60,000 IU/week for 6 weeks, 12.5% prescribe 2,000 IU/day for 3 months, while 4% give stat dose of 6 lac IU cholecalciferol.
78% (n = 75/95) of physicians evaluate for Vitamin D deficiency if an infant is hypocalcemic, while 22% do not evaluate all hypocalcemic children for Vitamin D deficiency. Of these, 4% evaluate if there is high alkaline phosphatase on investigation, 6% evaluate if clinical features of rickets present, 7% evaluate if symptomatic hypocalcemia, and 5% do not evaluate.
2/3rd (n = 62/96) of study population practices to check levels of 25 (OH) Vitamin D in serum in clinically diagnosed rickets and 62 of the 94 respondents believe X-ray should be done to diagnose rickets while 1/3rd do not use X-ray to diagnose rickets.
For treatment of NVDD, cholecalciferol is the preferred medicine for therapy among most of the respondents (94%). Out of all the study participants, 92% give RDA dose of Vitamin D after treatment. Majority (84%) physicians monitor children while on treatment for NVDD.
As the treatment for NVDD begins, the need of judgment for adequacy of treatment was asked. Physicians commented that they practice to monitor following parameters to know if adequate response to therapy is obtained – 32% follow-up children with X-ray alone, 15.6% follow-up with serum Calcium, Phosphate, and Alkpo4 levels, 11.4% follow-up with combination of above parameters.
About 58% (n=56/95) of physicians do not refer children with NVDD rickets for orthopedic intervention, 32.3% (n=31/95) refer, while 8% refer for opinion not necessarily intervention.
Physicians were asked about preparations, they use for calcium and Vitamin D supplementation. About 49% prescribe calcium carbonate containing formulation, while 34.4% prescribe calcium phosphate formulation. Out of 86 respondents of this question, 60 physicians have correctly specified content of formulation in mg/5 mL of calcium and/ or Vitamin D3 while 13 had variance in their knowledge of composition and 13 did not specify composition.
Overall responses were compared between consultant pediatricians (n = 50) versus residents (n = 46) [Table 3], then an intragroup analysis was also performed to compare responses across three categories in the consultant group, that is, fellows (n = 25), super-specialists (n = 9), and general pediatricians (n = 16) [Table 4]. No significant difference was found between the study groups.
| S. N. | Attitude and practice | Response | Resident n (%) | Consultant Pediatrician n (%) | Total no of respondents out of 96 | P value |
|---|---|---|---|---|---|---|
| 1. | Vitamin D to exclusively breastfed infant | Yes | 45 (97.83%) | 45 (90%) | 95 | 0.267 |
| 2. | Do you evaluate mother with NVDD child | Yes | 38 (82.61%) | 39 (78%) | 91 | 0.847 |
| 3. | Do you treat mother with NVDD child | Yes | 39 (84.78%) | 39 (78%) | 91 | 0.695 |
| 4. | Do you evaluate for 25(OH) D deficiency in infant with hypocalcemia | Yes | 32 (69.57%) | 43 (86%) | 95 | 0.059 |
| 5. | Do you give single mega dose of cholecalciferol | No | 41 (89.13%) | 39 (78%) | 96 | 0.144 |
| 6. | Do you give RDA after treatment of NVDD | Yes | 44 (95.65%) | 44 (88%) | 95 | 0.346 |
| 7. | Do you always do X-ray to diagnose rickets | Yes | 34 (73.91%) | 28 (56%) | 94 | 0.110 |
| 8. | Do you always check 25(OH) D levels in child clinically diagnosed with rickets | Yes | 27 (58.7%) | 35 (70%) | 96 | 0.247 |
| 9. | Do you monitor while on treatment | Yes | 41 (89.13%) | 40 (80%) | 96 | 0.218 |
| 10. | Do you refer children with rickets for orthopedic intervention | Yes No Maybe |
14 (30.43%) 29 (63%) 2 (4.35%) |
17 (34%) 27 (54%) 6 (12%) |
95 | 0.362 |
| S. N. | Attitude and practice | Response | Fellow n (%) | General pediatrician (%) | Pediatric superspecialist n (%) | Total no of respondents out of 50 | P value |
|---|---|---|---|---|---|---|---|
| 1. | Vitamin D to exclusively breastfed infant | Yes | 24 (96%) | 14 (87.5%) | 7 (77.78%) | 49 | 0.212 |
| 2. | Do you evaluate mother with NVDD child | Yes | 19 (76%) | 13 (81.25%) | 7 (77.78%) | 47 | 0.779 |
| 3. | Do you treat mother with NVDD child | Yes | 19 (76%) | 13 (81.25%) | 7 (77.78%) | 47 | 0.779 |
| 4. | Do you evaluate for 25(OH) D deficiency in infant with hypocalcemia | Yes | 21 (84%) | 14 (87.5%) | 8 (88.89%) | 49 | 0.905 |
| 5. | Do you give single mega dose of cholecalciferol | No | 19 (76%) | 11 (68.75%) | 9 (100%) | 50 | 0.183 |
| 6. | Do you give RDA after treatment of NVDD | Yes | 23 (92%) | 12 (75%) | 9 (100%) | 49 | 0.503 |
| 7. | Do you always do X-ray to diagnose rickets | Yes | 16 (64%) | 8 (50%) | 4 (44.44%) | 48 | 0.705 |
| 8. | Do you always check 25(OH) D levels in child clinically diagnosed with rickets | Yes | 19 (76%) | 10 (62.5%) | 6 (66.67%) | 50 | 0.636 |
| 9. | Do you monitor while on treatment | Yes No |
22 (88%) | 13 (81.25%) | 5 (55.56%) | 50 | 0.112 |
| 10. | Do you refer children with rickets for orthopedic intervention | Yes No May be |
9 (36%) 5 (60%) 1 (4%) |
5 (31.25%) 9 (56.25%) 2 (12.5%) |
3 (33.33%) 3 (33.33%) 3 (33.33%) |
50 | 0.222 |
DISCUSSION
India is a tropical country well placed under the brightly shining Sun. Vitamin D is a sunshine hormone, synthesized under the skin with the help of ultraviolet rays of the sunlight easily available to most of us. Despite this, Vitamin D deficiency is an epidemic in India because of many factors like higher melanin in skin acting as a natural sunscreen, overcrowding, pollution, urbanization restricting sunlight exposure, and socioreligious practices. Hence, clinical assessment and supplementation of Vitamin D become important along with creating awareness among parents and treating physicians for well-being of children.
Response rate in the survey was excellent (93%). Our study revealed that physicians have a fair knowledge about NVDD. About 75% of physicians are aware of epidemic nature of Vitamin D deficiency. Inadequacy of dietary sources in providing the vitamin is also well known in majority of study participants, that is, 93.8%. Out of all, 92.71% of physicians have noted the subclinical nature of Vitamin D deficiency as well as other subtle clinical symptoms such as muscle weakness, tiredness, and irritability. Importance of calcium supplementation during treatment phase of Vitamin D deficiency was agreed on by 93.75% of physicians. On knowledge regarding recent definition, RDA and therapeutic dosage positive responses were variable, that is, 35.4%, 62.5%, and 40%, respectively. This data highlighted the area with scope for further improvement in knowledge of physicians.
The attitude and practices of physicians are basically guided by their knowledge, thus reflected positive attitude related to supplementation of RDA of Vitamin D to breastfed infants (93.4%), evaluation of hypocalcemic infant s (78%), and evaluation and treatment of mother of Vitamin D deficient child (81%). 2/3rd of study population practices to check levels of 25 (OH) Vitamin D in serum for clinically diagnosed rickets, 2/3rd diagnose rickets based on X-ray features.
In a similar study conducted by Mekonnen et al., about knowledge, attitude, and practice of healthcare workers (HCW) on measuring adult Vitamin D level, diagnosing deficiency, and managing consequent health conditions in three ecologies of Ethiopia, suggested a little over half of HCWs have good knowledge and close to two-thirds of them have positive attitude while less than half of them have good practice on adult Vitamin D deficiency[14] which is comparable to our study which showed that –
About 49% of physicians had a knowledge score of more than 11 and 51% had a score between 7 to 10
About 2% of physicians had an attitude and practice score of <10, 36% of physicians had a score between 10 to 15, and 62% of physicians had a >15 positive attitude score.
These numbers are higher than those reported by two other studies – one study conducted on knowledge, attitude, and practice of General pediatricians in Dammam, Saudi Arabia, toward Vitamin D supplementation to infants[15] and another study recording response regarding the importance of Vitamin D and calcium among undergraduate health sciences students in Al Kharj, Saudi Arabia, which revealed that undergraduate health science students were familiar with the importance of Vitamin D and calcium; however reported improper attitude that warranted further health guidance and educational programs.[16]
CONCLUSION
The study identifies the gaps in the knowledge of physicians about the epidemic nature of NVDD, definition, and treatment protocols. It recognizes the inconsistency in identification, diagnosis, treatment, and prevention protocols across all study groups.
The study additionally reveals that healthcare workers with good knowledge and a positive attitude have a better practice of Vitamin D service provision.
To reach a consensus and avoid confusion regarding the definition, investigation of Vitamin D deficiency, and its treatment, better attention should be given to design appropriate guidelines considering the experiences of all physicians in diagnosis and treatment of this condition. It is essential to create adequate awareness at all levels of the health-care system for better outcomes of NVDD in the pediatric population.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Worldwide Vitamin D status. Best Pract Res Clin Endocrinol Metab. 2011;25:671-80.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D nutritional status of exclusively breast fed infants and their mothers. J Pediatr Endocrinol Metab. 2009;22:241-6.
- [CrossRef] [PubMed] [Google Scholar]
- Sunlight exposure and development of rickets in Indian toddlers. Indian J Pediatr. 2010b;77:61-5.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D and the immune system: New perspectives on an old theme. Endocrinol Metab Clin N Am. 2010;39:365-79.
- [CrossRef] [PubMed] [Google Scholar]
- Cellular and molecular effects of Vitamin D on carcinogenesis. Arch Biochem Biophys. 2012;523:107-14.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D levels and early mortality among incident hemodialysis patients. Kidney Int. 2007;72:1004-13.
- [CrossRef] [PubMed] [Google Scholar]
- Association of Vitamin D status with arterial blood pressure and hypertension risk: A mendelian randomisation study. Lancet Diabetes Endocrinol. 2014;2:719-29.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D and diabetes: Let the sunshine in. Diabetes Educ. 2008;34:939-40, 942, 944 passim
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D and hypertension. Electrolyte Blood Press. 2017;15:1-11.
- [CrossRef] [PubMed] [Google Scholar]
- Global consensus recommendations on prevention and management of nutritional rickets. J Clin Endocrinol Metab. 2016;101:394-415.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge, attitude and practice of health care workers on measuring adult Vitamin D level, diagnosis of deficiency, and management of consequent health conditions in three ecologies of Ethiopia: A cross-sectional study. BMC Nutr. 2020;6:77.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge, attitude, and practice of General pediatricians in Dammam, Saudi Arabia towards Vitamin D supplementation to infants. J Family Community Med. 2015;22:135-9.
- [CrossRef] [PubMed] [Google Scholar]
- Response regarding the importance of Vitamin D and calcium among undergraduate health sciences students in Al Kharj, Saudi Arabia. Arch Osteoporos. 2020;15:114.
- [CrossRef] [PubMed] [Google Scholar]




