
Translate this page into:
Role of magnetic resonance angiography in moyamoya syndrome in a child with sickle cell anaemia

*Corresponding author: Nidhi Aggarwal, Department of Radiology, Bai Jerbai Wadia Hospital for Children, Mumbai, Maharashtra, India. drnidhi.aggarwal1811@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Aggarwal N, Gala F. Role of magnetic resonance angiography in moyamoya syndrome in a child with sickle cell anaemia. Wadia J Women Child Health. 2024;3(1):50-1. doi: 10.25259/WJWCH_46_2023
A 16-year-male with sickle cell anemia presented with the right-sided hemiparesis and right focal seizures for past 3 years. He was referred to our department for magnetic resonance imaging of brain which showed chronic gliotic infarcts in the bilateral frontoparietal region (left more than right) [Figure 1a-b]. Magnetic resonance time-of-flight angiography showed reduced flow in bilateral internal carotid arteries throughout their course (left more than right) with occlusion of terminal internal carotid arteries [Figure 2a]. Reduced flow was also seen in bilateral middle and anterior cerebral arteries with paucity of cortical branches. Multiple leptomeningeal and basal collaterals were seen with prominent flow in bilateral external carotid arteries and posterior circulation [Figure 2b-c]. Moyamoya disease is an idiopathic, often familial, condition causing steno-occlusive intracranial vascular changes. Similar vascular changes secondary to causes such as atherosclerosis, phacomatosis, vasculitis, and blood dyscrasias are moyamoya phenomenon or syndrome. It should be considered in case of sickle cell anemia presenting with neurological deficits.
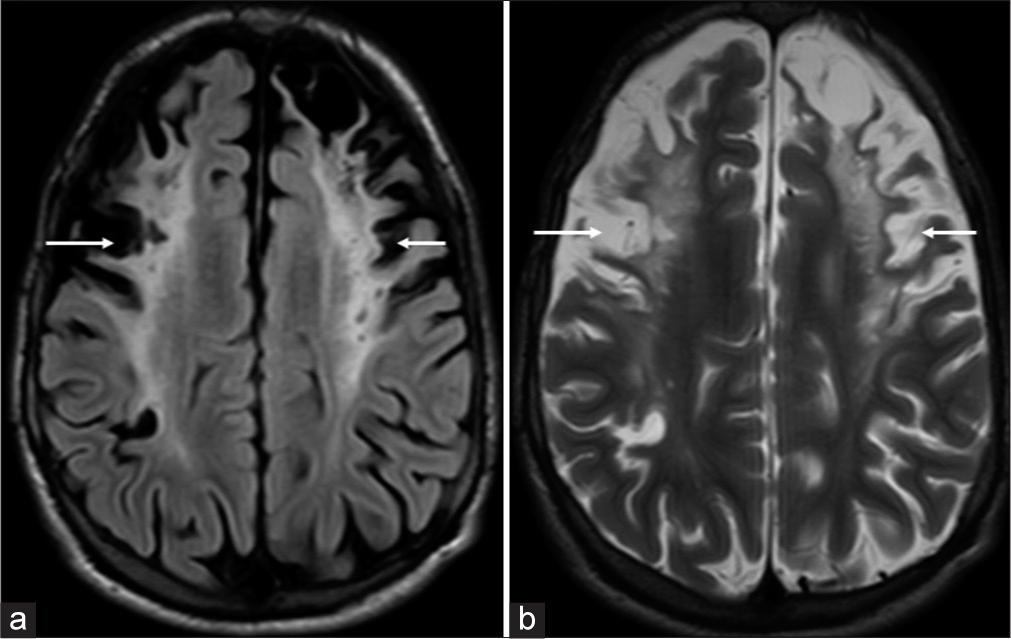
- (a) Axial fluid-attenuated inversion recovery and (b) T2-weighted images showing areas of gliosis with encephalomalacia in bilateral frontoparietal lobes (white arrows in a and b).
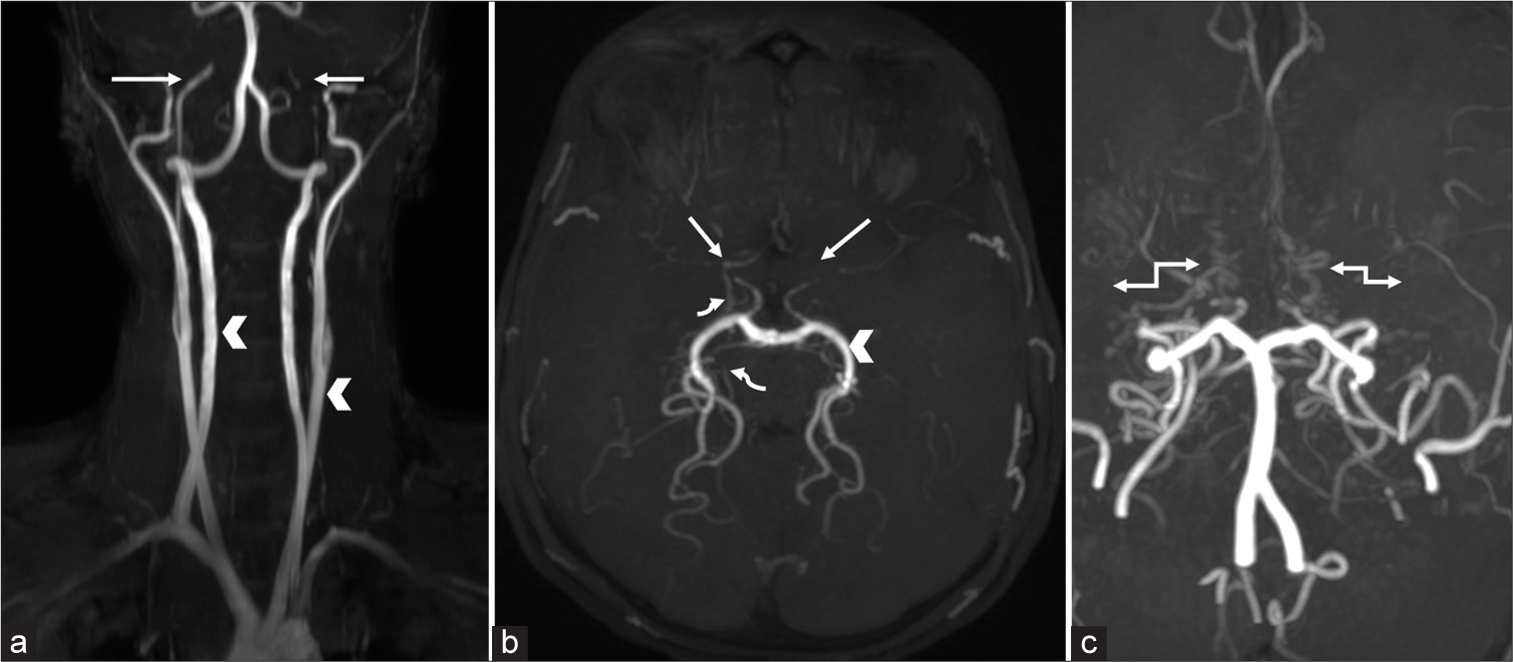
- Coronal (a) magnetic resonance time-of-flight angiography of neck show normal vertebral and common carotid arteries (white arrowheads). Bilateral internal carotid arteries are narrowed from origin to throughout entire course with occlusion of terminal segments (white arrows). Axial magnetic resonance time-of-flight angiography of brain (b) shows thin narrowed bilateral middle and anterior cerebral arteries (straight white arrows). Prominent posterior circulation (white arrowhead) and thin basal and perimesencephalic collaterals (curved white arrows) are seen. Coronal magnetic resonance time-of-flight angiography of brain (c) showed thin basal collaterals mimicking “puff of smoke appearance” (double headed white arrows).
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.




