
Translate this page into:
Recurrent subdural hematoma as presentation of neonatal biliary atresia: A case report
*Corresponding author: Krishnan Nagarajan, Department of Radio-Diagnosis, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India. drbharathj16@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bharath J, Nagarajan K, Naseera M, Govindarajan K. Recurrent subdural hematoma as presentation of neonatal biliary atresia: A case report. Wadia J Women Child Health 2023;2(2):79-82.
Abstract
Biliary atresia is a congenital disorder of progressive and obliterative cholangiopathy, the most common cause of neonatal cholestasis, it can cause secondary vitamin-K deficiency bleeding due to the malabsorption of lipids and lipid-soluble vitamins due to cholestasis. We report a 46-day-old child presenting with cholestatic features complicated by subdural hematoma (SDH) and cerebral edema. On investigations, she was found to be having primary biliary atresia, for which she was operated but had a recurrence of the SDH on the opposite side.
Keywords
Subdural hematoma
Biliary atresia
Vitamin K deficiency
Neonatal bleeding diathesis

INTRODUCTION
Primary or extrahepatic biliary atresia is an obliterative cholangiopathy presenting in the 1st or 2nd month of life with jaundice, pale stools, and high-colored urine. Rarely, these children may present with complaints of bleeding. Cholestasis is associated with fat malabsorption which leads to poor absorption of fat-soluble vitamins A, D, E and K. Poor absorption of vitamin K leads to an increased bleeding tendency in children with biliary atresia.[1-4] Intracranial hemorrhage, either parenchymal or even subdural has been reported as an initial manifestation of biliary atresia.[5-7] We report a 46-day-old child who presented with poor feeding for which imaging was done that showed subdural hematoma (SDH) with brain edema. Subsequent work-up revealed biliary atresia which was managed by Kasai Portoenterostomy.
CASE REPORT
A 46-day-old female infant was brought with complaints of bleeding from the umbilicus, passing pale stools and high colored urine. She had a refusal to feed, high-pitched cry and abnormal posturing. At birth, she was in neonatal intensive care for 5 days and had physiological jaundice for which she received phototherapy. On general examination she was lethargic and had icterus and pallor. On systemic examination, liver was palpable 3 cm below the costal margin. Initial laboratory investigations showed that hemoglobin was 5.7 g%, prothrombin time was 148 s, international normalized ratio was 13.81, and activated partial thromboplastin time was 71.2 s. Alpha fetoprotein was 2262 ng/mL and direct hyperbilirubinemia was noted. The screening test for Toxoplasmosis, Rubella, CMV, Herpes (TORCH) infections was negative. Reverse transcription polymerase chain reaction for COVID-19 infection was negative.
Due to her poor sensorium and posturing, a plain computed tomography (CT) brain was done that showed a large right SDH with diffuse white matter hypodensity in the right hemisphere and a thin SDH without mass effect on the left side. Magnetic resonance imaging (MRI) brain showed T1 and T2 hyperintense subdural collection in the bilateral convexities suggestive of subacute SDH [Figure 1]. Areas of diffusion restriction with subtle T2/fluid-attenuated inversion recovery (FLAIR) hyperintensity were noted involving the right cerebral hemisphere including internal capsule, splenium, and rostrum of the corpus callosum and right pyramidal tract.
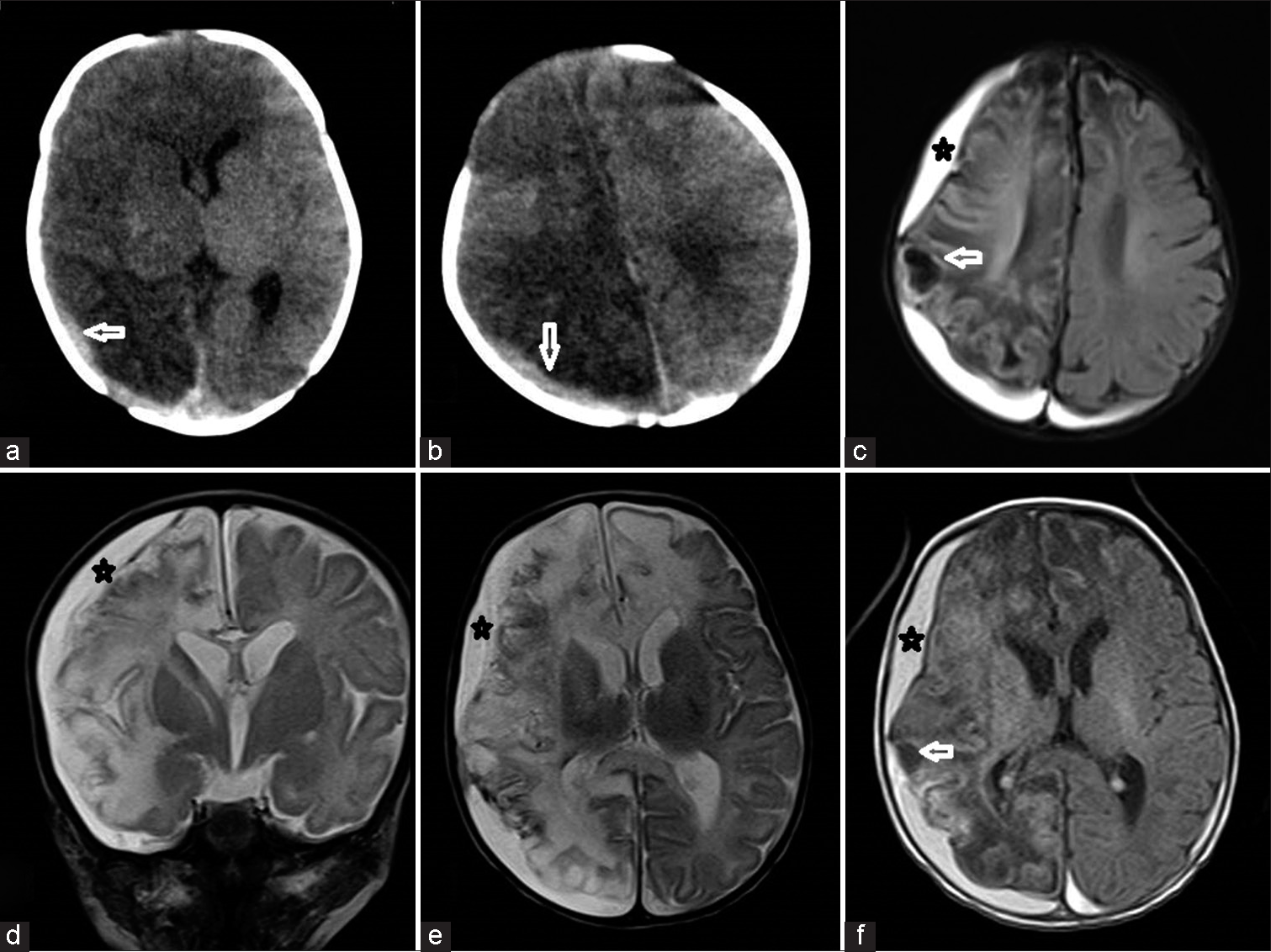
- Plain computed tomography sections (a and b) showing right temporoparietal subdural hematoma (SDH) with the right cerebral hemispheric edema. Magnetic resonance imaging fluid attenuated inversion recovery axial (c), T2 coronal (d), T2 axial (e), and T1-weighted axial (f) sections showing right frontotemporoparietal T1/T2 hyperintense subacute SDH with hemispheric edema and early gliotic changes.
Ultrasonography of the abdomen showed altered liver echogenicity and a small gallbladder with ill-defined margins. Nuclear cholescintigraphy with HIDA (hepatobiliary iminodiacetic acid) revealed mild to moderately impaired hepatocellular function with no excretion of contrast into the bowel for 24 hours suggestive of biliary atresia. After correction of coagulation profile, the patient was operated on Kasai portoenterostomy was done and liver biopsy was taken. The child was symptomatically better after the surgery and was discharged after 2 weeks. Liver biopsy showed features suggestive of biliary atresia. After 2 months, the child was again brought with poor sensorium and symptoms of raised intracranial pressure (ICP). CT brain showed right cerebral hemisphere gliosis and atrophy along with recurrent SDH on the right side with hyperdense fluid level [Figure 2]. The parents were not willing for another surgery after the abdominal portoenterostomy. CT brain done after 2 days showed reduction in mass effect with frontal lobe hypodensities. The child was conservatively managed and was discharged with some residual paucity of left-sided limb movements. Further follow-up after 3 months revealed recurrent SDH on the left frontoparietal convexity with gliosis of the right cerebral hemisphere, ventriculomegaly, and resolution of the right-sided subdural collection.
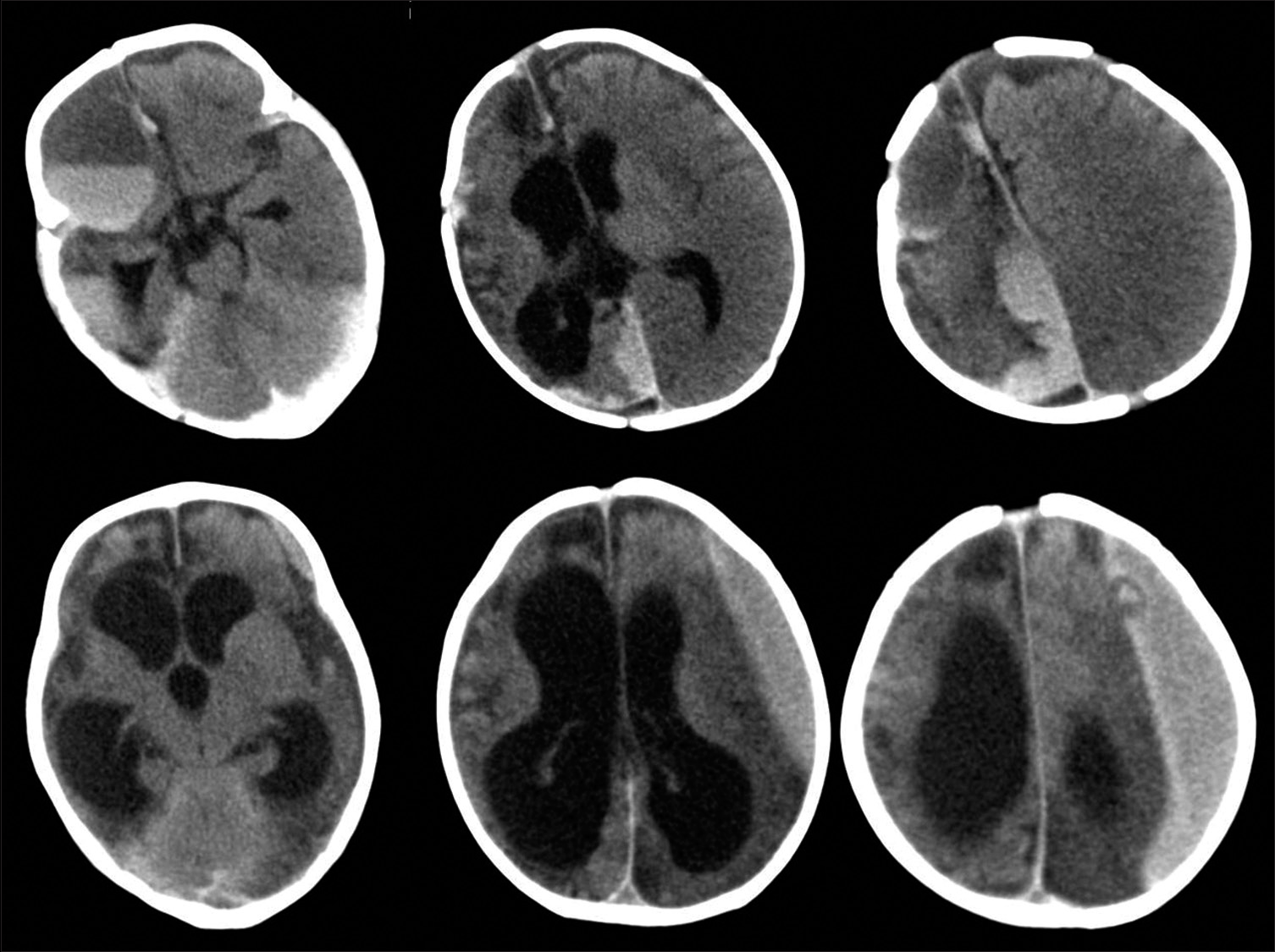
- Plain computed tomography (CT) brain shows acute-on-chronic mixed density subdural hematoma with fluid-level and extension along the interhemispheric fissure. Right cerebral hemiatrophy is noted due to gliosis resulting from the previous subdural hematoma (SDH). Follow-up CT after 3 months shows recurrent left frontoparietal SDH with right hemispheric gliosis and ventriculomegaly.
DISCUSSION
SDH in neonatal and infantile period can be due to many causes such as birth-related trauma, coagulopathy, maternal medications, and non-accidental injuries. There is higher risk of SDH in twins, preterm births, neonatal convulsions, or small-for-gestational age babies.[8] Feldman et al.,[9] in their prospective study of 66 children, found abusive injury as the cause in 39 (59%), accidental injury in 15 (23%), and indeterminate in 12 (18%). Hobbs et al.,[10] in an epidemiological study of SDH and effusions, found that out of 186 infants, 106 had non-accidental head injury, seven accidental head injury, 26 perinatal cause, 7 non-traumatic medical condition, 23 meningitis, 17 were undetermined and the deaths reported were 35.
The overall incidence of biliary atresia is approximately 1 in 10,000-16,000 live births.[7] Untreated children with biliary atresia often do not survive beyond 3 years of age. At present, the management is surgical and includes Kasai portoenterostomy. Even after successful surgery, progression to liver fibrosis and cirrhosis is frequently seen. Liver transplantation is the only treatment option for patients who develop liver cirrhosis, and biliary atresia is the one of the most common indications for pediatric liver transplantation.[3]
Vitamin K, a lipid-soluble vitamin, is a cofactor for activation of various coagulation factors (II, VII, IX, and X). Biliary atresia is associated with cholestasis-induced fat malabsorption and fat-soluble vitamins resulting in vitamin K deficiency (VKD) bleeding.[11] The incidence of bleeding manifestations is variable and rarely bleeding disorder may be the first manifestation of biliary atresia. During active development of the nervous system during infancy, there is accelerated neovascularization which may be related to the development of intracranial hemorrhage in these patients. Intracranial hemorrhage may lead to delayed developmental milestones, cerebral palsy, and mental retardation. Subdural and subarachnoid hemorrhages are more common than intraparenchymal hemorrhages.[4] However, the prophylactic administration of Vitamin K is found to be insufficient to prevent bleeding manifestations in infants with biliary atresia. This could probably be due to their higher bleeding propensities as a result of secondary late-type VKD from vitamin K malabsorption from the digestive tract.[7]
CONCLUSION
SDH may be a complication of cholestatic liver disease in infants and may not be fully corrected even after vitamin K supplementation due to secondary factors of malabsorption and breastfeeding. As the number of cases reported is less, it is uncertain whether continued vitamin K supplementation alone is useful.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Intracranial hemorrhage due to Vitamin K deficiency associated with congenital biliary atresia: A case report. Neurosurg Emerg. 2000;5:77-80.
- [Google Scholar]
- Bleeding disorder as the first symptom of biliary atresia. Eur J Pediatr Surg. 2005;15:295-9.
- [CrossRef] [PubMed] [Google Scholar]
- Image and diagnosis. Intracranial haemorrhage due to Vitamin K deficiency, as the first symptom of extrahepatic biliary atresia. West Indian Med J. 2005;54:392-397.
- [CrossRef] [Google Scholar]
- Intracranial hemorrhage and Vitamin K deficiency associated with biliary atresia: Summary of 15 cases and review of the literature. Pediatr Neurosurg. 2006;42:362-7.
- [CrossRef] [PubMed] [Google Scholar]
- Intracranial hemorrhage as initial presentation of biliary atresia: Two cases report. Arch Argent Pediatr. 2011;109:e119-21.
- [CrossRef] [PubMed] [Google Scholar]
- Intracerebral hemorrhage despite prophylactic administration of Vitamin K in infants--two case reports. Neurol Med Chir (Tokyo). 2011;51:130-3.
- [CrossRef] [PubMed] [Google Scholar]
- Subdural hemorrhage: A unique case involving secondary Vitamin K deficiency bleeding due to biliary atresia. Forensic Sci Intern. 2012;221:e25-9.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of subdural haemorrhage during infancy: A population-based register study. PLoS One. 2018;13:e0206340.
- [CrossRef] [PubMed] [Google Scholar]
- The cause of infant and toddler subdural hemorrhage: A prospective study. Pediatrics. 2001;108:636-46.
- [CrossRef] [PubMed] [Google Scholar]
- Subdural haematoma and effusion in infancy: An epidemiological study. Arch Dis Child. 2005;90:952-5.
- [CrossRef] [PubMed] [Google Scholar]
- Intracranial hemorrhage associated with Vitamin K-deficiency bleeding in patients with biliary atresia: Focus on long-term outcomes. J Pediatr Gastroenterol Nutr. 2012;54:552-7.
- [CrossRef] [PubMed] [Google Scholar]




