
Translate this page into:
From placenta to cradle: Histopathology as a predictor of fetal and neonatal well-being

*Corresponding author: Kiran More, Division of Neonatology, Madanmohan Ramnarain Ruia Children’s Hospital, Thane, Maharashtra, India. drkiranmore@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Srivastava R, More K. From placenta to cradle: Histopathology as a predictor of fetal and neonatal well-being. Wadia J Women Child Health. 2024;3:119-25. doi: 10.25259/WJWCH_5_2025
Abstract
Placental histopathology serves as an invaluable tool in understanding fetal and neonatal outcomes. This review synthesizes the current knowledge regarding various placental lesions, their clinical significance, and their correlation with neonatal morbidity and mortality. Through a detailed examination of placental structure, abnormalities, and histopathological findings, this article highlights the predictive potential of placental pathology in clinical practice. Emphasis is placed on how specific pathologies such as vascular malperfusion, chorioamnionitis, and villitis influence outcomes such as intrauterine growth restriction, preterm birth, and neonatal sepsis. Key findings from recent literature are integrated with histopathological examination protocols to propose a comprehensive framework for utilizing placental pathology in perinatal care.
Keywords
Fetus
Histopathology
Neonatal outcomes
Newborn
Placenta

INTRODUCTION
The placenta is a dynamic organ essential for fetal growth and development. It mediates gas exchange, nutrient transfer, and waste elimination between the mother and fetus. Placental pathologies can disrupt these functions, leading to adverse fetal and neonatal outcomes.[1] In clinical settings, histopathological examination of the placenta often provides critical insights into perinatal complications[2] and has good predictive potential in clinical practice.[3] Placental histopathology is important not only in understanding implantation and early pregnancy survival[4] but also in giving evidence of insufficiency and its clinical implications.[5] In addition, placental findings give significant insights into acute chorioamnionitis and funisitis, possible group B streptococcal neonatal sepsis,[6,7] and may be useful in situations such as preterm premature rupture of membranes.[8] Studies have also shown associations between placental disorders and conditions such as bronchopulmonary dysplasia and necrotizing enterocolitis in preterm infants, underscoring the necessity for comprehensive placental evaluation.[9]
Understanding these pathologies is essential for timely diagnosis and management, thereby enhancing maternal-fetal well-being and reducing risks associated with adverse pregnancy outcomes. Research has increasingly highlighted the intricate relationship between placental health and neonatal outcomes, with various pathologies linked to long-term infant development and immediate postnatal complications. As advancements in diagnostic methodologies and a deeper understanding of placental physiology emerge, the potential for optimizing care and outcomes for both mothers and infants remains significant.
This review article aims to synthesize current knowledge on placental lesions, their clinical significance, and their impact on fetal and neonatal health.
PLACENTAL STRUCTURE AND FUNCTION
The placenta comprises two main surfaces: The fetal surface, smooth and amnion-covered, and the maternal surface, which is dull, grayish-red, and divided into cotyledons. Its histological layers include the chorionic plate, basal plate, and intervillous space. Villi, categorized into primary, secondary, and tertiary stages, form the functional units responsible for the exchange between maternal and fetal blood. Any disruption in this architecture can result in compromised placental function, manifesting as pregnancy complications such as intrauterine growth restriction (IUGR), preterm birth, or stillbirth.[10]
CLASSIFICATION OF PLACENTAL LESIONS
Based on the Amsterdam Placental Workshop Group criteria,[11] placental lesions are classified into vascular processes, infectious-inflammatory processes, and other processes.
Vascular lesions
Fetal malperfusion is a critical aspect that underscores the importance of placental health in neonatal outcomes. Research has demonstrated a significant association between IUGR and fetal malperfusion, emphasizing the role of chronic hypoxia due to placental disorders.[12]
Poor villous development and abnormal branching of the placental villous tree are architectural hallmarks indicative of vascular-based fetal growth pathologies, which can lead to compromised fetal growth and subsequent adverse neonatal outcomes.
Some common conditions affecting fetal perfusion are as follows:
Maternal Vascular Malperfusion (MVM): These lesions are characterized by abnormalities such as infarcts, abruptio placentae, and maternal arterial atherosclerosis. They are key contributors to fetal hypoxia and are often associated with conditions such as pre-eclampsia and IUGR.[13]
Fetal Vascular Malperfusion (FVM): These include lesions like thrombi in chorionic vessels, avascular villi, and chorionic plate abnormalities. They can lead to fetal hypoxia and are linked to conditions such as thromboembolic events and umbilical cord accidents.[14]
Redline et al. detailed the histopathological criteria for MVM and FVM, emphasizing their clinical significance in adverse pregnancy outcomes.[13,14]
Infectious-inflammatory lesions
Inflammatory lesions within the placenta, categorized as acute or chronic, have significant implications for neonatal health. Acute inflammatory lesions indicate recent or active intrauterine infections, necessitating immediate evaluation and potential treatment for sepsis in newborns. Conversely, chronic inflammatory lesions may signal prolonged placental dysfunction, often linked to immune-mediated processes between the mother and fetus.[15]
Some common inflammatory conditions are as follows:
Maternal Chorioamnionitis: This condition is marked by inflammation of the chorion and amnion, typically resulting from bacterial infections ascending from the lower genital tract. It is often linked to preterm labor and neonatal sepsis.
Fetal Vasculitis: Characterized by inflammation of the fetal blood vessels within the placenta, it can lead to complications such as neonatal sepsis and chronic inflammatory responses.
Villitis of unknown etiology (VUE) is associated with viral infections and can contribute to fetal growth restrictions (FGRs) due to immune rejection mechanisms
Roberts et al. explored the inflammatory pathways involved in chorioamnionitis and their impact on neonatal health.[16]
Other lesions
Massive Perivillous Fibrin Deposition: This condition involves the extensive accumulation of fibrin around the placental villi, leading to placental insufficiency and adverse pregnancy outcomes such as IUGR and stillbirth.
Vilitis of unknown etiology (VUE): VUE is characterized by chronic inflammation of the placental villi, often recurring in subsequent pregnancies. It is associated with adverse outcomes such as IUGR and preterm birth.
Hecht et al. investigated the recurrent nature of VUE and its implications for pregnancy management.[17] By understanding these classifications, clinicians can better interpret placental findings and correlate them with clinical outcomes, thereby improving perinatal care and management.
CORRELATION OF SPECIFIC HISTOPATHOLOGIES WITH OUTCOMES
Understanding the correlation between specific placental histopathologies and neonatal outcomes is crucial for improving perinatal care. Various studies have explored these correlations, providing valuable insights into the impact of placental lesions on fetal and neonatal health [Table 1].[2]
Preterm Labor
|
Hypoxic-Ischemic Encephalopathy (HIE): Hypoxic conditions often result from abruptio placentae, umbilical cord accidents, or chronic placental malperfusion. Placental examination in HIE cases frequently reveals vascular thrombi and villous infarctions, underscoring the role of placental vascular integrity in fetal oxygenation.[2]
IUGR: Chronic MVM, characterized by villous infarctions and fibrin deposition, is a leading histopathological finding in IUGR cases. The presence of delayed villous maturation further accentuates the growth restriction.[2]
Preterm Birth: Histological chorioamnionitis is a predominant lesion in preterm deliveries. It triggers inflammatory cascades that weaken fetal membranes and precipitate preterm labor. Chronic inflammatory processes, including villitis, are also frequently observed.[2]
Stillbirth and Neonatal Mortality: Placental lesions, including severe vascular malperfusion and massive feto-maternal hemorrhage, are common in stillbirths. Pathologies such as placental abruption and umbilical cord abnormalities further contribute to these outcomes.[2] Figure 1 explains pathophysiological concept of inflammatory process affecting neonatal outcomes.
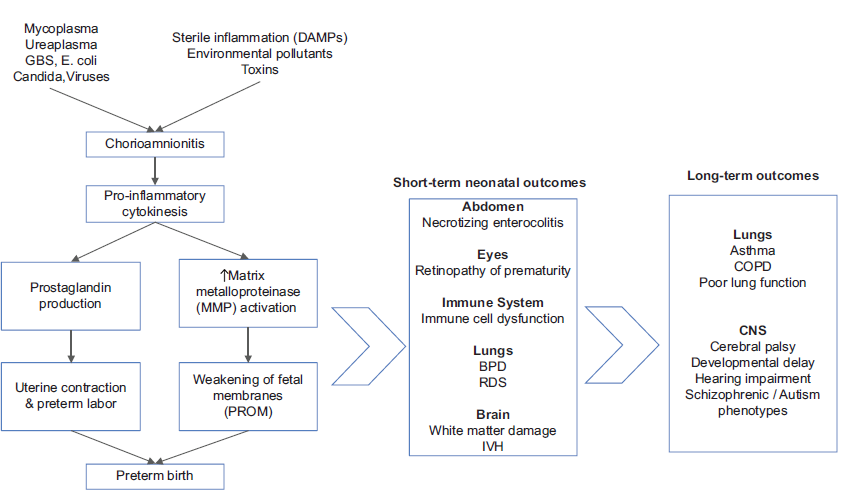
- Inflamatory process in chorioamnionitis and their neonatal impact. GBS: Group B Streptococcus, DAMP: Damage-associated molecular patterns, PROM: Premature rupture of membranes, BPD: Bronchopulmonary dysplasia, RDS: Respiratory distress syndrome, IVH: Intraventricular hemorrhage, COPD: Chronic obstructive pulmonary disease, CNS: Central Nervous System.
CLINICAL APPLICATIONS OF PLACENTAL HISTOPATHOLOGY
Histopathological examination of the placenta offers a systematic approach to investigating adverse outcomes. CAP guidelines recommend placental evaluation in cases of stillbirth, IUGR, preterm delivery, and neonatal complications such as sepsis.[18]
INDICATIONS OF PLACENTAL HISTOPATHOLOGY
Table 2 lists the indications for placental submission for histopathological evaluation as per the College of American Pathologists Guidelines [CAP].[18]
| Neonatal indications | Maternal indications | Placental indications |
|---|---|---|
| Admission in neonatal intensive care unit | Systemic disorders | Physical abnormalityinfarct, vascular thrombosis, retroplacental hematoma, abnormal coloration/odor |
| Stillbirth or perinatal death | Preterm delivery ≤34 weeks | Small or large placental size |
| Compromised clinical condition: any of the following, cord ph <7, Apgar score ≤6 at 5 min, PPV for >10 min after birth, Hct <35% | Peripartum infection | Umbilical cord lesionsthrombosis, torsion, true knots |
| Hydrops | Suspected congenital infections | Cord length <32 cm at term |
| IUGR | Severe oligohydramnios | Long cord >100 cm at term |
| Seizures | Unexplained or recurrent pregnancy complicationsIUGR, stillbirth, prematurity | Abnormalities of placental shape |
| Sepsis | Invasive procedure with suspected placental injury | |
| Major congenital anomalies | ||
| Discordant twins | ||
| Birth weight >95th percentile | Maternal diabetes |
IUGR: Intrauterine growth restriction, PPV: Positive pressure ventilation, Hct: Hematocrit
Clinicians, obstetricians and neonatologists should understand the importance of placental examination and include placental examination as part of their routine protocols. The algorithm for placental examination which is given in Figure 2[18] as per the College of American pathologists [CAP] guidelines.

- Algorithm for placental examination CAP guidelines (1997). CAP: College of American pathologists.
MICROSCOPIC EXAMINATION OF PLACENTA SAMPLES
In laboratory settings, placenta samples undergo both macroscopic and microscopic examinations. The macroscopic analysis involves evaluating the maternal surface, umbilical length, presence of hematomas, membrane transparency, and lobulation. Microscopic examination includes assessing for fibrosis, trophoblastic cells, villi, inflammation, and other pathological changes. Data from these assessments are meticulously recorded for further analysis.[19]
DISCUSSION
The integration of placental histopathology into perinatal care has transformed the understanding and management of pregnancy complications. By offering a microscopic evaluation of placental tissue, this practice uncovers vital insights into the etiology of adverse pregnancy outcomes, shaping interventions for current and future pregnancies.
One pivotal area illuminated by placental histopathology is MVM, a condition arising from defective remodeling of uteroplacental spiral arteries. MVM compromises placental blood flow and is associated with adverse outcomes such as FGR, pre-eclampsia, and stillbirth. Early detection through histopathological criteria outlined by Redline et al. has enabled preventive strategies, including low-dose aspirin prophylaxis and heightened antenatal surveillance, to reduce maternal and fetal risks.[20]
Infectious-inflammatory lesions are another significant category of placental pathology. These lesions include maternal chorioamnionitis and fetal vasculitis. Maternal chorioamnionitis is characterized by inflammation of the chorion and amnion, often due to bacterial infections ascending from the lower genital tract. This condition is commonly associated with preterm labor and neonatal sepsis. Histopathological examination of the placenta can reveal the presence and extent of inflammation, providing critical information for the management of both the mother and the neonate. Roberts et al.[16] explored the inflammatory pathways involved in chorioamnionitis and their impact on neonatal health. Fetal vasculitis, characterized by inflammation of fetal blood vessels, can lead to complications such as neonatal sepsis and chronic inflammatory responses.
The predictive value of placental histopathology extends beyond immediate neonatal outcomes, informing the management of future pregnancies. Women with a history of MVM or other placental abnormalities benefit from increased surveillance, early interventions, and tailored antenatal care in subsequent pregnancies. Studies by Norwitz and Fox et al.[4,5] underscore the importance of identifying recurrent placental pathology to optimize perinatal outcomes.
Despite these advances, significant gaps exist in standardizing placental examination protocols. Variability in histopathological reporting can hinder the consistency and utility of findings. Langston et al.[18] have emphasized the need for standardized protocols to ensure systematic evaluations and improve inter-institutional comparability. Moreover, rare conditions such as chronic histiocytic intervillositis (CHI) demand further research. CHI, associated with severe FGR and stillbirth, remains poorly understood. Hecht et al.’s exploration of CHI has underscored the pressing need for evidence-based management guidelines.[17]
Placental pathology findings have implications that extend beyond the neonatal period, offering insights into the child’s long-term health.[21] Conditions such as IUGR and preterm birth –frequently linked to placental insufficiency – are associated with an increased risk of chronic diseases later in life. Research demonstrates that IUGR predisposes individuals to hypertension, cardiovascular disease, and type 2 diabetes due to fetal programming alterations.[22]
Similarly, preterm birth correlates with long-term risks such as chronic kidney disease, neurodevelopmental disorders, and respiratory complications. Early identification of at-risk neonates, coupled with targeted interventions, can mitigate these risks and improve long-term outcomes.[23]
Integrating placental histopathology into routine clinical practice requires collaboration between obstetricians, pathologists, and pediatricians. Multidisciplinary teams can ensure that placental findings are accurately interpreted and appropriately integrated into clinical care. This collaborative approach can facilitate early identification of at-risk pregnancies, timely interventions, and improved neonatal outcomes. In addition, educating healthcare providers about the importance of placental histopathology and its clinical implications is crucial for its successful integration into perinatal care.
Emerging technologies offer promising avenues for enhancing placental diagnostics. Advanced imaging techniques, such as three-dimensional ultrasound and magnetic resonance imaging (MRI), provide detailed insights into placental structure and function. In addition, non-invasive testing of fetal and placental DNA in maternal blood holds potential for early detection of placental pathologies. Machine learning applications in placental imaging are also being explored to refine diagnostic accuracy and accelerate clinical decision-making.
Placental histopathology serves as a cornerstone in elucidating the etiology of adverse fetal and neonatal outcomes. Incorporating comprehensive placental evaluations into perinatal care can significantly enhance prognosis and guide therapeutic interventions.
Future research should focus on refining diagnostic criteria for placental lesions, developing standardized examination protocols, and investigating the underlying mechanisms of rare pathologies. Advancements in imaging techniques and molecular diagnostics hold promise for enhancing the accuracy and utility of placental histopathology. For instance, the use of advanced imaging modalities such as three-dimensional ultrasound and MRI can provide detailed insights into placental structure and function. Similarly, molecular techniques such as genomic and proteomic analysis can uncover the molecular basis of placental pathologies and identify potential therapeutic targets.
CONCLUSION
Integrating placental histopathology into perinatal care provides crucial insights into pregnancy complications and informs the management of future pregnancies. Standardized protocols and further research into rare pathologies are essential to enhance perinatal outcomes and mitigate long-term health risks for the child.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Study of morphological and histological changes of the placenta in normal and high-risk pregnancies and effect of pregnancy outcome. Int J Clin Diagn Pathol. 2021;4:14-6.
- [CrossRef] [Google Scholar]
- The correlation of placental histopathology with neonatal outcome. Trop J Path Micro. 2018;4:336-43.
- [CrossRef] [Google Scholar]
- Clinical correlates of histopathological entities of the placenta. Aust J Gen Pract. 2021;50:62-9.
- [CrossRef] [PubMed] [Google Scholar]
- Implantation and the survival of early pregnancy. N Engl J Med. 2001;345:1400-8.
- [CrossRef] [PubMed] [Google Scholar]
- The histopathology of placental insufficiency. J Clin Pathol Suppl (R Coll Pathol). 1976;10:1-8.
- [CrossRef] [PubMed] [Google Scholar]
- Significance of placental findings in early-onset group B streptococcal neonatal sepsis. Clin Pediatr (Phila). 1985;24:256-8.
- [CrossRef] [PubMed] [Google Scholar]
- Acute chorioamnionitis and funisitis: Definition, pathologic features, and clinical significance. Am J Obstet Gynecol. 2015;213:S29-52.
- [CrossRef] [PubMed] [Google Scholar]
- Placental histology and clinical characteristics of patients with preterm premature rupture of membranes. Obstet Gynecol. 1997;89:265-71.
- [CrossRef] [PubMed] [Google Scholar]
- Placental pathology, perinatal death, neonatal outcome, and neurological development: A systematic review. PLoS One. 2014;9:e89419.
- [CrossRef] [PubMed] [Google Scholar]
- Altered development and function of the placental regions in preeclampsia and its association with long-chain polyunsaturated fatty acids. Wiley Interdiscip Rev Dev Biol. 2016;5:582-97.
- [CrossRef] [PubMed] [Google Scholar]
- Sampling and definitions of placental lesions: Amsterdam placental workshop group consensus statement. Arch Pathol Lab Med. 2016;140:698-713.
- [CrossRef] [PubMed] [Google Scholar]
- The association of placental abruption and pediatric neurological outcome: A systematic review and meta-analysis. J Clin Med. 2023;12:205.
- [CrossRef] [PubMed] [Google Scholar]
- Maternal vascular underperfusion: Nosology and reproducibility of placental reaction patterns. Pediatr Dev Pathol. 2004;7:237-49.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical and pathological umbilical cord abnormalities in fetal thrombotic vasculopathy. Hum Pathol. 2004;35:1494-8.
- [CrossRef] [PubMed] [Google Scholar]
- Pregnancy complications, correlation with placental pathology and neonatal outcomes. Front Clin Diabetes Healthc. 2022;2:807192.
- [CrossRef] [PubMed] [Google Scholar]
- Antenatal infection and adverse pregnancy outcomes. Best Pract Res Clin Obst Gynaecol. 2010;24:339-49.
- [Google Scholar]
- Chronic histiocytic intervillositis: Clinical features and obstetric outcomes. Placenta. 2014;35:23-9.
- [Google Scholar]
- Practice guideline for examination of the placenta: Developed by the placental pathology practice guideline development task force of the college of American pathologists. Arch Pathol Lab Med. 1997;121:449-76.
- [Google Scholar]
- Leveraging the placenta to advance neonatal care. Front Pediatr. 2023;11:1174174.
- [CrossRef] [PubMed] [Google Scholar]
- Placental diagnostic criteria and clinical correlation-A workshop report. Placenta. 2004;25:S8-36.
- [Google Scholar]
- Histopathological study of placenta in high-risk pregnancies in a tertiary care center. Int J Med Pharm Res. 2024;5:348-53.
- [Google Scholar]
- Preterm birth, kidney function and cardiovascular disease in children and adolescents. Children. 2022;9:1130.
- [CrossRef] [PubMed] [Google Scholar]
- Prematurity, perinatal inflammatory stress, and the predisposition to develop chronic kidney disease beyond oligonephropathy. Pediatr Nephrol. 2021;36:1673-81.
- [CrossRef] [PubMed] [Google Scholar]




