
Anisocoria in a neonatal intensive care unit: An ophthalmological emergency?
*Corresponding author: R. R. Prashanth, Department of Neonatology, Indira Gandhi Institute of Child Health, Bengaluru, Karnataka, India. prash2635@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Prashanth RR, Nair S, Goyal M, Patel T, More T, Haribalakrishna A. Anisocoria in a neonatal intensive care unit: An ophthalmological emergency? Wadia J Women Child Health. 2024;3:148-50. doi: 10.25259/WJWCH_19_2024
A female neonate born at 33 weeks of gestation with a birth weight of 2000 g was referred to our center on the 15th day of life with Pseudomonas sepsis without meningitis. During evaluation for retinopathy of prematurity (ROP), the right eye showed a pupillary dilatation of 3 mm whereas the left pupil showed dilatation up to 1 mm, after mydriatic instillation [Figure 1]. There were multiple hypopigmented creamy lesions on both nasal and temporal sides sparing the macula in the right eye and the left fundus could not be visualized through partially dilated pupils. An urgent B scan showed no evidence of vitreitis. Bilateral fungal endophthalmitis was suspected and a systemic evaluation including repeat blood culture, cerebrospinal fluid analysis, echocardiography, renal ultrasound, and urine for fungal elements was negative. She was started on Injection Amphotericin B and topical medications including steroids, homatropine, timolol, and dorzolamide. She was followed up twice weekly with a B scan and fundus examination which showed resolving lesions on the right side with the formation of snowballs in the areas of hypopigmentation and reduction in vitreal haze. However, the left eye still could not be dilated beyond 2 mm. After completion of Injection Amphotericin B for 21 days, repeat fundus examination showed a large chorioretinal scar sparing the macula with multiple small scars in the nasal and temporal fundus in the left eye [Figure 1]. Repeat B scan showed no evidence of vitreitis. At present, the neonate is 2 months old on visual rehabilitation. Parents have been counseled regarded the guarded visual prognosis and the need for continued follow-up.
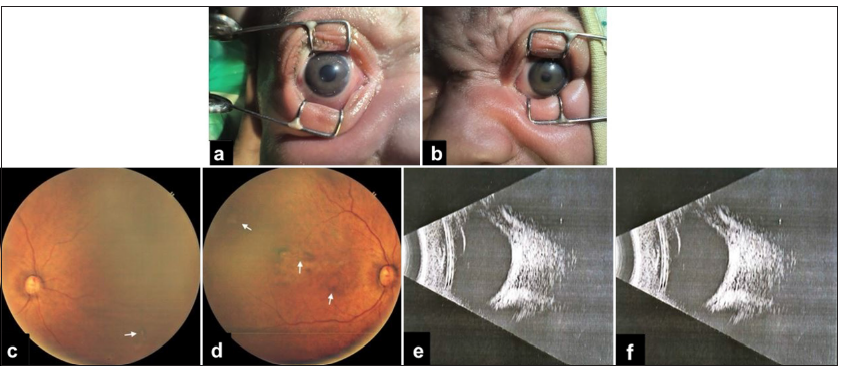
- (a) Anisocoria with the right eye showed a pupillary dilatation of 3 mm, (b) The left pupillary dilatation of up to one mm. (c) Fundus examination of right eye: Small scars in the nasal retina (white arrow), (d) Fundus examination of left eye: large chorioretinal scar sparing the macula with multiple small scars in the nasal and temporal fundus (white arrows). (e) B scan with no evidence of vitreitis in right eye, (f) B scan with no evidence of vitreitis in left eye.
Endophthalmitis is defined as suppurative inflammation of the internal structures of the eye. The primary site of infection includes the retina, choroid, and ciliary body secondary to the inherently increased blood flow. Although the etiology mainly consists of bacteria, the incidence of endogenous candida endophthalmitis (CE) with systemic candidemia varies from 6% to 50%.[1]
In CE, lesions are usually multiple and are bilateral in up to two-thirds of the cases. The hallmark findings include creamy white lesions in the chorioretinal region along with vitreous haze. Initially, the lesions appear flat, but the typical vitreous haze appears when these lesions further extend by penetrating the retinal barrier, giving an elevated appearance. These progressive lesions often heal with scarring, resulting in retinal traction and detachment. Vitreal abscesses are also a known presentation of CE, which appear as puff ball-like lesions in the vitreous cavity.[2]
CE may cause the release of proinflammatory cytokines that promote retinal neovascularization and the progression of ROP. Anisocoria as seen in the index case is an overlapping sign of ROP and one may miss an underlying endophthalmitis unless thoroughly investigated.[3]
The blood-ocular barrier plays a key role in deciding the mainstay of treatment in these cases. Although under normal conditions, it maintains a sterile environment in the interior of the eye, it also prevents the elimination of infections and affects the entry of systemically administered antibiotics. The blood-ocular barrier is usually broken down during endophthalmitis, permitting entry of systemic administered antibiotics into the eye and making them the mainstay of therapy with other strategies such as intravitreal antibiotics and vitrectomy being controversial.[4] Vitrectomy in children, especially neonates, is difficult due to anatomical challenges and is only attempted in the most severe cases with guarded prognosis with risk of complications such as retinal detachment, cataract, glaucoma, persistent vitreous hemorrhage, and posterior synechiae.[4]
The prognosis of CE is concerning, with mortality up to 50%, and the ophthalmologic prognosis of survivors being poor with retained intact vision in only two-thirds of neonates.[5] Given high mortality and vision loss, early detection of neonatal endophthalmitis, especially with an underlying fungal etiology in the neonatal intensive care units, should be treated as an ophthalmological emergency with additional emphasis on monitoring the size of pupils and reaction to light in sick preterm neonates.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Endogenous bacterial endophthalmitis: A 17-year prospective series and review of 267 reported cases. Surv Ophthalmol. 2003;48:403-23.
- [CrossRef] [PubMed] [Google Scholar]
- Fungal endophthalmitis In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559257 [Last accessed on 2024 May 01]
- [Google Scholar]
- Severe bacterial endophthalmitis: Towards improving clinical outcomes. Expert Rev Ophthalmol. 2010;5:689-98.
- [CrossRef] [PubMed] [Google Scholar]
- 25-Gauge vitrectomy for paediatric vitreoretinal conditions. Br J Ophthalmol. 2009;93:787-90.
- [CrossRef] [PubMed] [Google Scholar]
- Neonatal endogenous endophthalmitis: A report of six cases. Pediatrics. 2013;131:e1292-7.
- [CrossRef] [PubMed] [Google Scholar]




