
Translate this page into:
A rare case of conservatively managed congenital chylothorax presenting as hydrops fetalis
*Corresponding author: R. R. Prashanth, Department of Neonatology, Indira Gandhi Institute of Child Health, Bengaluru, Karnataka, India. prash2635@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Subhash A, Prashanth RR, Bandiya P, Shivanna N. A rare case of conservatively managed congenital chylothorax presenting as hydrops fetalis. Wadia J Women Child Health. 2024;3:141-5. doi: 10.25259/WJWCH_44_2024
Abstract
We report a term female neonate with non-immune hydrops fetalis with bilateral pleural effusion diagnosed as congenital chylothorax. Bilateral chest tube drainage is done and the neonate is successfully managed with measures including mechanical ventilation, medium chain triglyceride milk-based diet, and injection octreotide. A detailed course in the neonatal intensive care unit with a literature review on the management of congenital chylothorax has been included.
Keywords
Non-immune hydrops
Chylothorax
Pleural effusion

INTRODUCTION
Non-immune hydrops fetalis (NIHF) is a complication of congenital chylothorax occurring due to the accumulation of chyle. Overall, 753 such cases have been reported, with 68% of them being managed conservatively.[1] The cause of this could be due to abnormalities of the lymphatic system, including lymphangiectasia, which is seen in 79% of cases.[2]
CASE REPORT
A female neonate, born at 37 weeks to a 35-year-old mother with multiple gestation and nonconsanguineous union, had normal prenatal ultrasounds until the second trimester; further scans were not conducted. Delivery occurred through lower segment cesarean section due to a previous cesarean. The neonate did not cry immediately after birth and required extensive resuscitation, which included chest compressions and one dose of adrenaline. The APGAR scores were 2 and 4 at 1 and 5 min, respectively.
In the delivery room, the neonate was noted to have anasarca: Temperature: 98.6°F (36.5°C), heart rate: 170 beats per minute, respiratory rate: 76 breaths per minute, blood pressure: 60/42, mean 48 mmHg, and oxygen saturation: 65%. She was referred to our institution on bag and tube ventilation.
Upon arrival, the neonate had respiratory distress, hypoxia, and shock, weighing 2500 g (with edema), measuring 43 cm (3rd centile) in length and head circumference of 31.5 cm (3rd centile), with anasarca, ascites and diminished air entry on both sides. There was no pallor, dysmorphic facies, or hepatosplenomegaly, and the cardiovascular assessment was unremarkable. The baby was stuporous, hypotonic and a depressed neonatal reflexes.
The baby was kept on mechanical ventilation and inotrope support. The blood group of both mother and neonate was O positive and direct coombs test (DCT) was negative.
Differential diagnoses for NIHF including chromosomal abnormalities (Monosomy X, Trisomy 21, or Trisomy 18), congenital lymphangiectasia, congenital lung malformation, congenital chylothorax, intrauterine infection, and cardiovascular disorders such as structural heart disease, cardiomyopathy, and fetal arrhythmias were considered.
The details of the evaluation of non-immune hydrops have been summarized in Table 1.
| Lab investigation | Patient value | Normal reference range |
|---|---|---|
| Complete blood count | ||
| Hemoglobin (g %) | 20.4 | 13.4–23.7 |
| PCV (%) | 57.6 | 45–65 |
| MCV (fL) | 112 | 90–112 |
| MCH (pg) | 39.3 | 32.5 |
| MCHC (%) | 35.1 | 32.1 |
| RDW (%) | 16.0 | 16.18±1.23 |
| Retic count (%) | 6% | 0–1 |
| Total leukocyte count (cells/mm3) | 24500 | 5000–20000 |
| Platelet (lakhs/mm3) | 1.12 | 1.5–4.7 |
| Peripheral smear | Normocytic, normochromic blood picture | |
| Blood group | O positive | |
| Bone marrow examination | Not done | |
| Direct comb test | Negative | |
| Blood culture | No growth | |
| Liver enzymes | ||
| SGOT (U/L) | 62.3 | 9–80 |
| SGPT (U/L) | 12.1 | 13–45 |
| Total proteins (g %) | 3.3 | 6–7.5 |
| Serum albumin (g %) | 2.1 | 3–5 |
| Serum Urea | 28.0 | |
| Serum Creatinine | 0.7 | |
| Serum ammonia (mcg/mL) | 56 | 0.75–1.96 |
| Serum lactate (mmol/L) | 48 | 0.5–2.2 |
| TSH (μIU/mL) | 11 | Up to 20 |
| Total T4 | 6.47 | |
| Free T4 | 1.54 | |
| TORCH Titer | Negative | |
| Urine for proteins | Negative | |
| Skeletal survey | Normal | |
| Chest Xray | Bilateral pleural effusion | |
| Echocardiography | Normal | |
| Cranial Ultrasound | Normal | |
| Ultrasound abdomen and KUB | Normal | |
| Ophthalmology evaluation | Normal | |
| Karyotype | 44+xx | |
| OAE/AABR | Pass | |
PCV: Packed cell volume, MCV: Mean corpuscular volume, MCH: Mean corpuscular hemoglobin, MCHC: Mean corpuscular hemoglobin concentration,RDW: Red cell distribution width, OAE: Otoacoustic emission, AABR: Automated auditory brainstem response, TSH: Thyroidstimulating hormone, SGOT: Serum glutamic oxaloacetic transaminase, SGPT: Serum glutamic pyruvic transaminase, KUB: Kidney ureter bladder, TORCH: Toxoplasmosis, rubella, cytomegalovirus and herpes.
Chest X-ray and ultrasound revealed bilateral pleural effusion without any pericardial effusion [Figure 1]. Emergency pleural tapping was performed on both sides. Fifty milliliters of straw-colored fluid was aspirated from the left side and forty milliliters from the right side, after which a bilateral intercostal drainage (ICD) tube was inserted. This tube continued to drain straw-colored fluid, measuring 200 mL on the left side and 100 mL on the right side over the next 3 days [Figure 2]. The neonate was started on parenteral nutrition, including protein at 2 g/kg/day on day of life (DOL) 1, along with donor human milk and the mother’s own milk, which was increased to 30 mL/kg/day. On DOL 5, the pleural effusion worsened, and the ICD fluid changed from straw colored to milky white, increasing in quantity [Figure 3]. This issue was resolved upon changing the milk to medium-chain triglyceride (MCT)-based formula on DOL 7. The feed volume was gradually increased to 150 mL/kg/day with a targeted protein intake of at least 3.5–4 g/kg/day. Injection octreotide was considered due to persistently high mean airway pressure on ventilator and increasing ICD output over 4 days following which the ICD output significantly reduced. She also developed late-onset sepsis on DOL 3, which was managed with intravenous antibiotics. The neonate required high-frequency ventilation for the first 2 days, followed by conventional ventilation, and was removed from respiratory support by DOL 11. The baby achieved adequate weight gain from day 7 of life, and repeat blood counts and protein levels were normal.
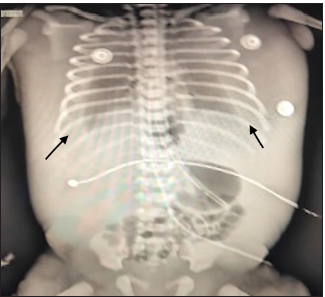
- X-ray showing bilateral pleural effusion (black arrows).

- Intercostal drainage showing thick straw color fluid suggesting lymphatic fluid.

- Intercostal drainage showing milky chylous fluid (black arrow) upon introduction of human milk.
The course in the hospital along with the details of pleural fluid cytology and biochemical analysis have been summarized in Table 2 [Figure 4].
| DOL 1 | DOL3 | DOL5 | DOL8 | DOL 11 | |
|---|---|---|---|---|---|
| Hb (g%) | 20.2 | 16 | 17.8 | 17.2 | 16.2 |
| TLC (cells/mm3) | 24.5 | 14.9 | 8.1 | 9.2 | 8.2 |
| Platelet (lakhs/mm3) | 1.12 | 1.05 | 1.08 | 1.64 | 1.72 |
| Chest Xray | Bilateral large pleural effusion [Figure 1] | Minimal bilateral effusion with ICD in situ | Minimal bilateral effusion with ICD in situ [Figure 4] | ||
| ICD drain color | Yellow straw | Yellow straw | Milky white | Milky white | ICD drain –minimal strawcolored |
| Pleural fluid analysis | Cells1360 All lymphocytes TG 34.8 |
Cells5000 N10 L90 TG182 |
Cell1200 N15 L85 |
||
| S. Triglycerides (mg/dL) | 46 | 133 |
DOL: Day of life, Hb: Hemoglobin, TLC: Total leukocyte count, N: Neutrophils, L: Lymphocytes, ICD: Intercostal drainage, TG: Triglycerides, S.: Serum

- Chest X-ray showing improvement in bilateral pleural effusion at the time of discharge.
Bilateral ICDs were removed on DOL-25 and discharged on MCT-based feeds. She is currently 48 days old and weighing 2900 g. Genetic testing is currently deferred for financial constraints and a magnetic resonance imaging brain is planned on follow-up.
DISCUSSION
The loss of chyle, a major source of proteins including albumin, immunoglobin lymphocytes, and triglycerides, predisposes the neonate to extrauterine growth restriction and increased risk of sepsis as in the index neonate.[3]
The management of such a neonate often starts in the labor room with antenatally detected cases being benefited by ex utero intrapartum treatment procedure and those diagnosed postnatally require extensive resuscitation and early chest tube drainage and mechanical ventilation including high-frequency oscillatory ventilation.[4,5]
These neonates are at risk of shock secondary to hypovolemia necessitating adequate fluid resuscitation and the need to keep nil per oral and to decrease the further accumulation of chyle; this necessitates the initiation of total parenteral nutrition.[6] The initial appearance of the chyle in the index case was clear straw-colored fluid and changed to a milky appearance after starting feeds. This is due to a progressive increase in the concentration of triglycerides in chyle in neonates who are fed. Availability of skimmed breast milk is a challenge and the use of MCT-based milk as the initial milk of choice in such neonates is an area of research interest.[7]
Octreotide decreases the secretion of pancreatic, biliary, and intestinal fluids; inhibits gallbladder contraction and gastrointestinal motility; and reduces splanchnic blood flow. Because of these physiological actions, octreotide may be used to lower portal pressure, fat absorption, and lymphatic flow in the thoracic duct in cases of congenital chylothorax. As in the index case, the use of octreotide is often limited to cases requiring prolonged mechanical ventilation (average 7 days) and its use safety, efficacy, and dosing regimens for neonatal patients with chylothorax need further studies.[8]
Antenatal recognition of such cases often leads to better delivery room preparation. Antenatal interventions such as pleurodesis with injection OK 432 have shown promising short-term results.[9,10]
Infants with chylothorax are at risk for hypoalbuminemia, electrolyte imbalances, clotting dysfunction, lymphopenia, anemia, and immune deficiency due to chronic immunoglobulin loss, which increases the likelihood of infections. A study by Caserio et al. involving 29 infants (1990–2006) reported no recurrence, with most remaining asymptomatic, although 27% developed asthma early on. Follow-up at an average age of 7 years also showed no recurrence. Developmental outcomes in these infants are influenced by associated anomalies or severe prematurity.[11,12]
This case highlights that a neonate diagnosed with NIHF, who typically experiences significant respiratory distress at birth along with bilateral pleural effusion and anasarca, should raise the possibility of congenital chylothorax. Both pleural tapping and ICD drainage are essential for diagnosing and treating these conditions. Initiating human milk feeds could exacerbate chylothorax, making MCT-based feeds a suitable alternative. It is crucial to anticipate and promptly manage sepsis and extrauterine growth restriction in these infants. The best approach for conservative management and avoiding surgery in such neonates includes parenteral nutrition, adequate ventilatory support, and octreotide to promote early recovery and discharge.
CONCLUSION
Congenital chylothorax requires a multidisciplinary approach to management. Nutritional considerations in neonates are paramount, particularly regarding the administration of breast milk and MCT-based formulas. Timely diagnosis and prompt treatment facilitate early discharge and ensure adequate growth in these neonates.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Congenital chylothorax of the newborn: A systematic analysis of published cases between 1990 and 2018. Respiration. 2022;101:84-96.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital chylothorax: A prospective nationwide epidemiological study in Germany. Arch Dis Child Fetal Neonatal Ed. 2015;100:F169-72.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital chylothorax. Semin Fetal Neonatal Med. 2017;22:234-9.
- [CrossRef] [PubMed] [Google Scholar]
- Management of congenital chylothorax of the newborn. Respiration. 2022;101:795-6.
- [CrossRef] [PubMed] [Google Scholar]
- Ventilation mode and outcome of premature infants with congenital chylothorax. J Matern Fetal Neonatal Med. 2012;25:1627-30.
- [CrossRef] [PubMed] [Google Scholar]
- Management and outcomes of congenital chylothorax in the neonatal intensive care unit: A case series. Pediatr Investig. 2017;1:21-25.
- [CrossRef] [PubMed] [Google Scholar]
- Mother's milk technicians: A new standard of care. J Hum Lact. 2013;29:323-7.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of congenital chylothorax with octreotide in a hydropic preterm infant. Paediatr Int Child Health. 2013;33:116-9.
- [CrossRef] [PubMed] [Google Scholar]
- A review of fetal thoracoamniotic & vesicoamniotic shunt procedures. J Obstet Gynecol Neonatal Nurs. 2012;41:426-33.
- [CrossRef] [PubMed] [Google Scholar]
- Intrapleural injection of OK-432 as the primary in-utero treatment for fetal chylothorax. Hong Kong Med J. 2012;18:156-9.
- [Google Scholar]
- Congenital chylothorax: From foetal life to adolescence. Acta Paediatr. 2010;99:1571-7.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital chylothorax: Antenatal intervention, survival, and outcome. Pediatr Neonatol. 2016;57:85-6.
- [CrossRef] [PubMed] [Google Scholar]




