
Translate this page into:
Weak left upper limb pulse! Could be anomalous origin of left subclavian artery
*Corresponding author: Siddhartha Jayantkumar Joshi, Department of Pediatric Cardiology, The Mission Hospital, Durgapur, West Bengal, India. dr.siddharthajoshi@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bangalia D, Nayak HK, Bhattacharjya S, Joshi SJ, Paul A. Weak left upper limb pulse! Could be anomalous origin of left subclavian artery. Wadia J Women Child Health. 2024;3(1):25-7. doi: 10.25259/WJWCH_6_2024
Abstract
A rare but treatable condition of anomalous origin of the left subclavian artery (LSCA) from the left pulmonary artery (LPA) notoriously causes subclavian steal syndrome and pulmonary steal syndrome. We present two cases of anomalous origin of LSCA, from pulmonary artery, their modes of presentation, cardiac evaluation and management with a brief review of literature.
Keywords
Anomalous origin of left subclavian artery
Right aortic arch
TOF
Aortic arch anomaly
Weak pulse

INTRODUCTION
Isolated left subclavian artery (ILSA) arising from the left pulmonary artery (LPA) with right aortic arch with congenital heart diseases (CHD) is a very rare anomaly. According to the literature review, incidence of right sided aortic arch is 0.05-0.1% of general population. ILSA constitutes 0.8% of all right-sided aortic arch anomalies of which 60% are a conotruncal anomaly.[1] Here, we report two cases of ILSA in pediatric population associated with tetralogy of fallot (TOF).
CASE SERIES
Case 1
A 17-year-old female presented with complaints of bluish discoloration of the body and easy fatiguability with intermittent claudication in her left hand. On clinical examination her upper limb pulses were weak. 2D Echocardiography was suggestive of TOF with a right aortic arch with an abnormal origin of the left subclavian artery (LSCA) which was further confirmed on cardiac catheterization [Figure 1]. She underwent intra-cardiac repair (ICR) for TOF with reimplantation of LSCA to the left common carotid artery resulting in better blood pressure and adequate pulses in left arm and on follow up, she is doing well.
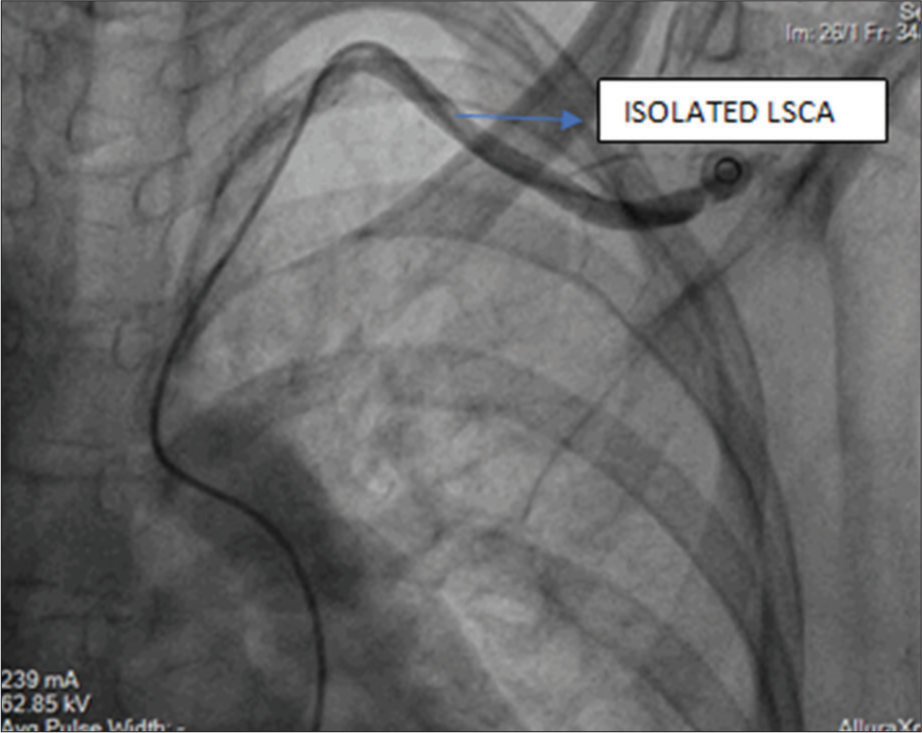
- Selective LSCA angiogram in AP View. catheter course: IVC - RA-RV-MPA-LPA - Ductus arteriosus - LSCA. LSCA: Left subclavian artery, AP: Antero-posterior, IVC: Inferior venacava, RA: Right atrium, RV: Right ventricle, MPA: Main pulmonary artery, LPA: Left pulmonary artery
Case 2
A 2-month-old baby presented with an incidental finding of ejection systolic murmur at left upper sternal border with weak left upper limb pulse and oxygen saturation of 93% in room air. 2D echocardiography was suggestive of TOF with the right sided aortic arch with suspicion of abnormal origin of LSCA from LPA with retrograde flow to LPA [Figure 2]. On further evaluation by computed tomography (CT) pulmonary angiography the diagnosis of TOF with the right aortic arch with anomalous LSCA from LPA, along with crisscross pulmonary arteries was confirmed [Figure 3]. The patient has been kept in follow-up for future surgical correction.

- Suspicion of abnormal origin of left subclavian artery from left pulmonary artery with retrograde flow to LPA in 2D echocardiography. LPA: Left pulmonary artery, LSCA: Left subclavian artery.
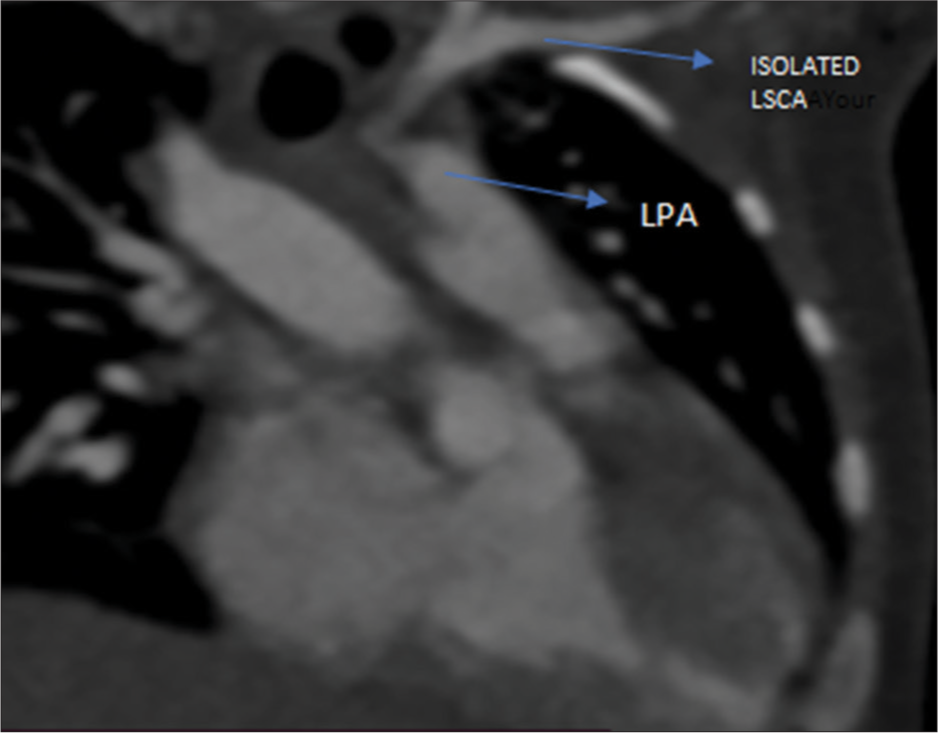
- Cardiac CT angio showing isolated left subclavian artery connected to LPA through ductus arteriosus. LPA: Left pulmonary artery, LSCA: Left subclavian artery.
DISCUSSION
The right aortic arch with ILSA is the rarest type of right aortic arch anomaly. Edward suggested that this anomaly results from the interruption of the left aortic arch at two locations: (1) between the left carotid and LSCA and (2) distal to the attachment of the left ductus arteriosus. So, the left subclavian artery does not have a connection with aorta, but it is connected to pulmonary artery by left ductus [Figure 4].[2,3]
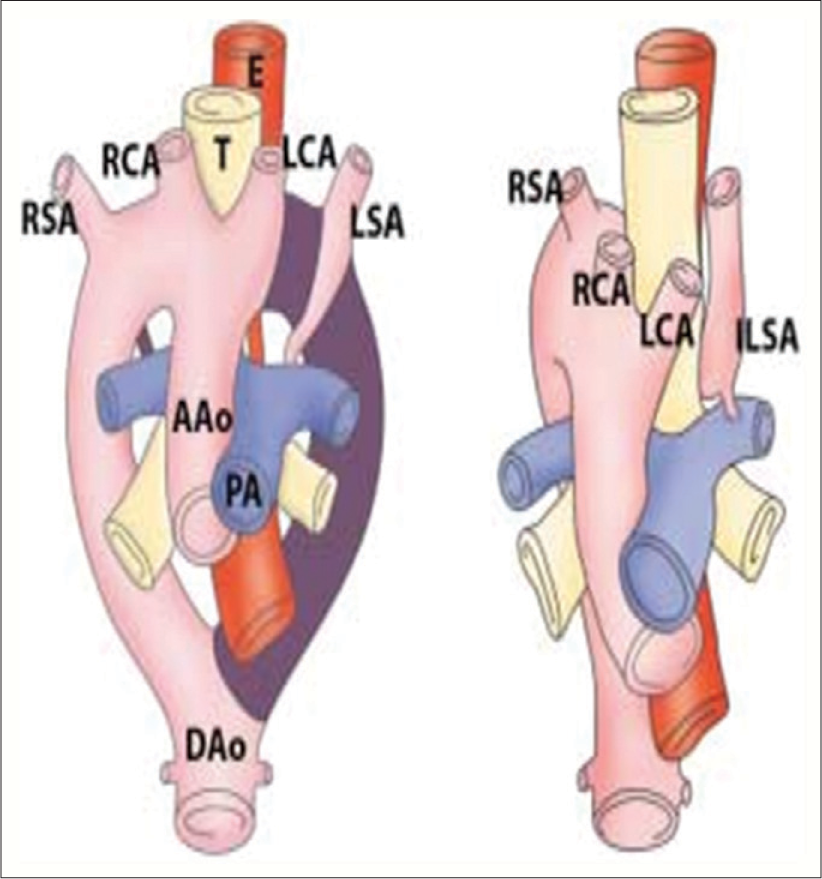
- Diagram of development of right aortic arch with isolated left subclavian artery is shown. Anomaly results from interruption of aortic arch at two level one level is between left common carotid and left subclavian arteries and other level is distal to left ductus. Left subclavian artery does not have connection with aorta but is connected to pulmonary artery by left ductus arteriosus. RSA: Right subclavian artery, RCA: Right carotid artery, T: Trachea, LCA: Left common carotid artery, LSA: Left subclavian artery, AA: Ascending aorta, PA: Pulmonary artery, DA: Descending aorta, E: esophagus, ILSA: isolated left subclavian artery.
Luetmer and Miller found that 23 out of 39 cases with isolated LSCA were having congenital heart disease. TOF was found in 14 out of 23 patients and double outlet right ventricle and d- Transposition of the great arteries (D-TGA) were other reported associated features in some cases.[4]
The clinical presentation of patients with ILSA depends on the patency of ductus arteriosus. They are mostly asymptomatic and usually detected during evaluation of heart disease or when reduced blood pressure is noted in the left upper limb. Although weak left upper limb pulses are commonly seen in coarctation of aorta and aortic arch interruption, they also have weak lower limb pulses.[5] Vertebrobasilar insufficiency occurs when the direction of blood flow is from left vertebrobasilar artery to the pulmonary artery (pulmonary steal syndrome) or the subclavian artery (subclavian steal syndrome).[6] Symptoms of insufficiency may include disturbance of vision, syncope, and headache that can be exacerbated by exercising the left upper limb. Patient with the pulmonary steal phenomenon is at risk of pulmonary over-circulation. Ischemic symptoms of the left arm, including pain weakness, coldness, and a reduced limb length, may be present.[7] Over time, asymptomatic patients loose the ability to compensate for the steal phenomenon and eventually become symptomatic with age.[7,8]
The optimal therapeutic approach is still undecided. Simple ligation of the LSCA, surgical re-implantation and device occlusion of the patent ductus arteriosus (PDA) have been described as therapeutic options. Many authors have suggested that simple ligation of LSCA or PDA is effective. However, persistence-isolated LSCA, not surgically reimplanted into the aorta, provides an anatomic defect for a subclavian steal syndrome.[7] In our case, the LSCA was directly anastomosed with the LCCA to prevent symptomatic subclavian or pulmonary steal.
CONCLUSION
Since ILSA is a rare anomaly, it can be easily missed during clinical examination and echocardiography. Hence, a high degree of suspicion is required during echocardiographic assessment of conotruncal abnormality with the right aortic arch. The anomaly can be confirmed by additional imaging such as cardiac CT or cardiac catheterization.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Isolation of left subclavian artery with reversal of neurological and hemodynamic abnormalities after percutaneous closure. Indian Heart J. 2014;66:477-80.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital anomalies of the aortic arch: Evaluation with the use of multidetector computed tomography. Korean J Radiol. 2009;10:176-84.
- [CrossRef] [PubMed] [Google Scholar]
- Anomalies of the derivatives of the aortic arch system. Med Clin North Am. 1948;32:925-49.
- [CrossRef] [PubMed] [Google Scholar]
- Right aortic arch with isolation of the left subclavian artery: Case report and review of the literature. Mayo Clin Proc. 1990;65:407-13.
- [CrossRef] [PubMed] [Google Scholar]
- Coarctation of the Aorta In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430913/ [Last assessed on 2023 Aug 08]
- [Google Scholar]
- Subclavian and pulmonary steal phenomenon in isolated left subclavian artery with left lung agenesis. Jpn Heart J. 2002;43:429-32.
- [CrossRef] [PubMed] [Google Scholar]
- Isolation of the left subclavian artery with right aortic arch in association with bilateral ductus arteriosus and ventricular septal defect. Korean J Thorac Cardiovasc Surg. 2015;48:415-8.
- [CrossRef] [PubMed] [Google Scholar]
- Abnormal origin of the left subclavian artery from the left pulmonary artery in a patient with double outlet right ventricle. The Korean Journal of Thoracic and Cardiovascular Surgery. 2014;. ;47:32.
- [CrossRef] [PubMed] [Google Scholar]




