
Translate this page into:
Vulvar donovanosis – An unusual cause of genital ulcer in a female
*Corresponding author: Sharmila Vijayan, Department of Obstetrics and Gynecology, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. sharu_jipmer@yahoo.co.in
-
Received: ,
Accepted: ,
How to cite this article: Balakrishnan P, Vijayan S. Vulvar donovanosis – An unusual cause of genital ulcer in a female. Wadia J Women Child Health 2023;2(2):83-5.
Abstract
Genital ulcer is one of the common complaints which is encountered among adolescent and adult patients. Amongst the various causes, donovanosis is a rare entity due to the widespread use of antibiotics. Most of the genital ulcers are diagnosed clinically and treated empirically. Some need further evaluation when they do not respond to empirical treatment. Diagnosis is often delayed due to late presentation, lack of suspicion, use of inappropriate diagnostic investigations, and the treatment is challenging due to antibiotic resistance. We are presenting a case of vulvar donovanosis in a 40-year-old female diagnosed with cytopathology due to its rare incidence in this advanced antibiotic era.
Keywords
Donovanosis
Genital ulcer
Cytopathology
Granuloma inguinale
Klebsiella granulomatis

INTRODUCTION
Donovanosis, also known as granuloma inguinale or granuloma venereum, is a sexually transmitted infection caused by Klebsiella granulomatis (previously known as Calymmatobacterium granulomatis), a Gram-negative bacteria.[1,2] It is a chronic progressive granulomatous ulcer affecting labia minora and fourchette in females and prepuce, glans penis, and coronal sulcus in males.[1,2] It was initially described by McLeod in 1882.[2] We are reporting a case of vulvar donovanosis in a 40-year-old female diagnosed by cytopathology.
CASE REPORT
A 40-year-old parous perimenopausal lady presented to the gynecology department with swelling over the vulva for 5 months duration which was painless, non-itching, and not associated with any discharge. It started as a small papule and progressed to a present lesion in 5 months. There was no history of trauma, vaginal discharge, itching, or bleeding per vagina. There was no history of human immunodeficiency virus (HIV), tuberculosis, or extramarital sexual contact. There was no history of similar complaints in her husband. On clinical examination, she had an ulcerated vulvar mass measuring 4 × 4 cm which was non-tender, not indurated, and was associated with active serosanguinous discharge. There was no inguinal lymphadenopathy. Per vaginal examination was normal. Considering differential diagnoses of infectious and neoplastic causes of vulvar ulcer, a smear from serosanguinous discharge and a Pap smear was taken. HIV serology was also done, which was non-reactive. Pap smear was negative for intraepithelial lesion or malignancy. Cytopathological examination of discharge smear stained with Giemsa stain showed macrophages containing Donovan bodies which are dark blue safety pin-shaped bipolar Gram-negative bacteria [Figure 1]. Diagnosis of donovanosis was made by the presence of Donovan bodies in the cytoplasm of macrophages. The diagnosis was confirmed by histopathological examination of ulcer edge biopsy which also ruled out malignancy. The patient was treated with azithromycin 1 g orally, weekly once for 4 weeks regimen, and she responded to treatment well.
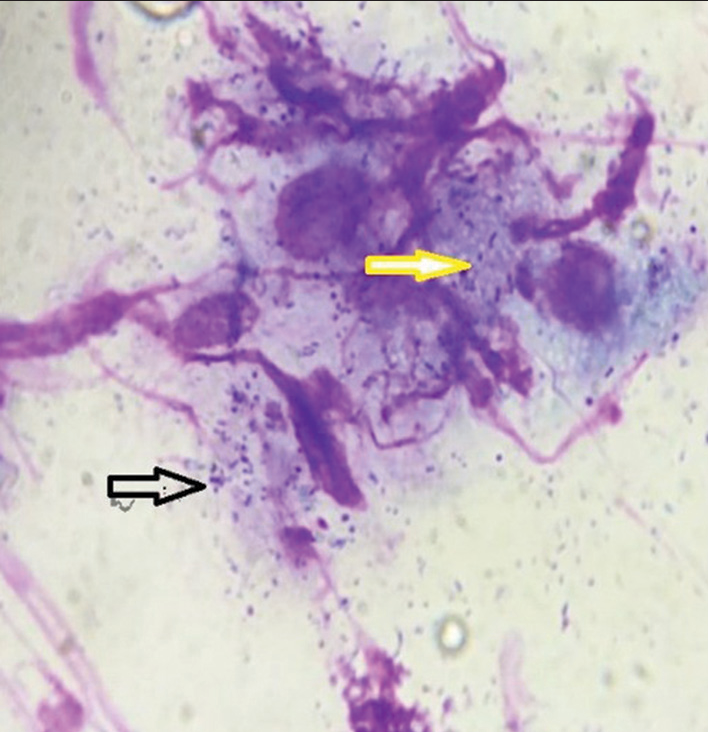
- Cytology smear shows intracellular (macrophages) (yellow arrow) and extracellular Donovan bodies (black arrow) (Giemsa stain, 100×).
DISCUSSION
The most common route of transmission of the organism causing donovanosis is sexual followed by fecal contamination and autoinoculation; however, our patient denied sexual promiscuity.[1] The disease usually starts as a small papule and then progresses to a nodule and ulcerated mass with a beefy red fleshy surface [Figure 2a and b].[1,3] Based on the appearance, there are four clinical variants-fleshy, sclerotic, hypertrophic, and rapidly destructive lesion.[4] Our case presented with a painless ulcerated vulvar mass similar to cases described in the literature.[1,5] Cases with extragenital lesions of donovanosis were also reported involving the oral cavity, vertebra, etc.[6,7] Since K. granulomatis cannot be cultured, the gold standard method of diagnosing donovanosis is tissue biopsy stained with Giemsa stain showing Donovan bodies in macrophages as demonstrated in our case, which also screens for the presence of malignancy.[1,2,5] Donovan bodies are ovoid- or bean-shaped bacteria and have a closed safety pin appearance on Giemsa staining due to the presence of blue chromatin inclusions at each pole.
![Clinical images from literature. (a) Photograph showing large bleeding ulcer over the right labia with the arrow pointing to the bubo over the right inguinal region in an 18-year-old girl.[1] (b) A 44-year-old male with AIDS had a penile ulcer for 8 months.[3] These patients were diagnosed with granuloma inguinale on evaluation.](/content/147/2023/2/2/img/WJWCH-2-083-g002.png)
- Clinical images from literature. (a) Photograph showing large bleeding ulcer over the right labia with the arrow pointing to the bubo over the right inguinal region in an 18-year-old girl.[1] (b) A 44-year-old male with AIDS had a penile ulcer for 8 months.[3] These patients were diagnosed with granuloma inguinale on evaluation.
Various treatment regimens are available with azithromycin, doxycycline, cotrimoxazole, ciprofloxacin, and erythromycin. The regimen should be selected based on the antibiotic sensitivity of the organism for prompt response.[3,8] Early diagnosis and appropriate treatment help in preventing complications, such as pseudoelephantiasis of the vulva and malignant transformation which necessitates vulvectomy.[2,9] Cases of transformation of vulvar donovanosis ulcer into squamous cell carcinoma have been reported emphasizing the importance of diagnosis of the cause of genital ulcer.[1,2,5]
CONCLUSION
We diagnosed a case of vulval donovanosis in a 40-year-old patient who presented with an ulcerated vulvar mass by histopathologic examination. A clinician should consider donovanosis as one of the differential diagnoses while treating a patient with a genital ulcer in order to prevent a fatal malignant transformation of the lesion.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- A forgotten disease reminds itself with a rare complication. Indian J Dermatol. 2011;56:430-1.
- [CrossRef] [PubMed] [Google Scholar]
- A clinical and investigational study of donovanosis. Indian J Dermatol Venereol Leprol. 2003;69:159-62.
- [Google Scholar]
- Nonhealing genital ulcer in AIDS: A diagnostic dilemma! Indian J Sex Transm Dis AIDS. 2016;37:197-200.
- [CrossRef] [PubMed] [Google Scholar]
- Donovanosis; granuloma inguinale, granuloma venereum. Monogr Ser World Health Organ. 1954;24:1-72.
- [Google Scholar]
- Genital donovanosis with malignant transformation: An interesting case report. Indian J Sex Transm Dis AIDS. 2014;35:135-7.
- [CrossRef] [PubMed] [Google Scholar]
- Disseminated donovanosis (granuloma inguinale) causing spinal cord compression: Case report and review of donovanosis involving bone. Clin Infect Dis. 1998;26:379-83.
- [CrossRef] [PubMed] [Google Scholar]
- The Centers for Disease Control and Prevention (CDC) 2015. Available from: https://www.cdc.gov/std/treatment-guidelines/genital-ulcers.htm [Last accessed on 2021 Jul 22]
- [Google Scholar]
- Donovanosis (granuloma inguinale) with vulval pseudo-elephantiasis. P N G Med J. 1982;25:283-5.
- [Google Scholar]




