
Translate this page into:
A novel and effective technique to exteriorise large uteri during laparotomic hysterectomy and myomectomy
*Corresponding author: Payal D. Lakhani, Department of Obstetrics and Gynaecology, Nowrosjee Wadia Maternity Hospital, Mumbai, Maharashtra, India. payal_lakhani@rediffmail.com
-
Received: ,
Accepted: ,
How to cite this article: Lakhani PD. A novel and effective technique to exteriorise large uteri during laparotomic hysterectomy and myomectomy. Wadia J Women Child Health 2022;1(1):29-30.
Abstract
Laparotomic hysterectomy commonly referred to as abdominal hysterectomy becomes an especially challenging procedure in large uteri namely size equivalent or larger than 20 weeks size gravid uterus. The biggest challenge in such cases is to exteriorize the uterus from the incision prior to starting with the surgical steps. This case report demonstrates the use of a silastic vacuum cup with a vacuum machine to facilitate the exteriorization of uterus from a regular Pfannenstiel incision.
Keywords
Laparotomic hysterectomy
Vacuum cup
Exteriorization

INTRODUCTION
Traditionally large incisions are used to facilitate the exteriorization of the uterus during abdominal hysterectomy thereby allowing better exposure and manipulation of the uterus. These incisions are infra umbilical midline vertical incisions, large rectus muscle cutting or splitting incisions like Maylard’s or Cherney’s incisions.
Manipulation of the uterus would require manual traction or use of a myoma screw. Surgeons often remove the most accessible fibroid without exteriorizing the uterus in an attempt to debulk the uterus following which it becomes relatively easier to exteriorize the uterus. However this leads to hemorrhage and distortion of the anatomy.
Use of a vacuum cup offers multiple advantages like reduction in size of the incision, reduction in use of traumatic instruments or traction sutures, reduction in hemorrhage and post-operative pain. The use of a vacuum cup to aid the exteriorization of the uterus will eliminate all the above maneuvers. An additional advantage is the prevention of trauma to the serosal or muscularis layer of the uterus during manipulation.[1] This step represents advantages in terms of carcinogenic safety.
CASE REPORT
A hysterectomy was being performed for a 49-year-old lady with a large 16 cm posterior uterine wall fibroid with adenomyosis documented on sonography. Clinically the uterus was equivalent to a 20 weeks size gravid uterus.

- Application technique
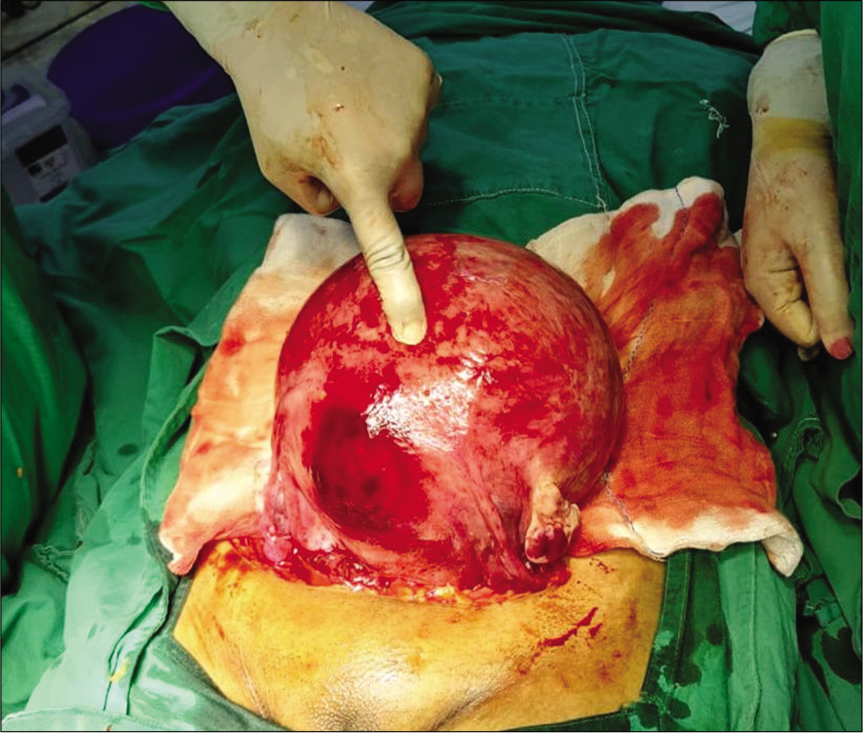
- Appearance of the exteriorized uterus after use of vacuum
After making a Pffanensteil incision, the operative field was cleared of bowel and omentum and a 6 cm diameter silastic vacuum cup was used with a traditional pressure gauge suction machine. The vacuum cup was attached to the most accessible and prominent portion of the fibroid and uterine fundus. Pressure was built up to 600 mm Hg and traction applied along the incision line and also cephalo-caudally.
After visualizing a large part of the posterior uterine wall fibroid, the suction was released and the cup was re applied to the fibroid. Repeat traction led to a smooth delivery of the large uterus out of the abdominal incision. The hysterectomy steps were started as standard technique and surgery completed in 1 h 10 min.
DISCUSSION
A vacuum cup is an instrument used to facilitate the delivery of the fetus during vaginal deliveries in cases of mild cephalo-pelvic disproportions or in cases where second stage of labor has to be cut short and delivery of the fetus expedited.
The same principle of cephalo-pelvic disproportions led to the use of this technique in abdominal hysterectomy whereby the intention is to deliver out a large uterus from a regular incision without trauma.
The larger abdominal incisions come with a risk of increased hemorrhage and post-operative pain along with increased operative time.
This relatively novel technique avoids the use of instruments like myoma screws which cause trauma and hemorrhage and also breach in the serosa and muscularis layer of the uterus which may post a carcinogenic threat in cases of undetected uterine cancers or malignant fibroids.
The only precautions that need to be taken during this procedure is to clear out the area where the vacuum cup is to be applied of bowel loops or omentum.
The challenges while using this procedure would be in multiple uterine fibroids with a bosselated appearance of the uterus which makes it difficult for the vacuum cup to get attached and negative pressure created.
However, various sizes of silastic vacuum cups are available which may be selected according to the uterine size and appearance.
CONCLUSION
This technique enhances patient safety and surgeon comfort during abdominal hysterectomy or myomectomy and also reduces tissue manipulation and organ damage.
Acknowledgments
Administration and Staff of Nowrosjee Wadia Maternity Hospital.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflict of interest.
References
- An original and effective technique to improve exposure in open surgery. Gynecol Surg. 2017;14:10.
- [CrossRef] [PubMed] [Google Scholar]




